

- See:
- Anterior Approach to the Shoulder
- Discussion:
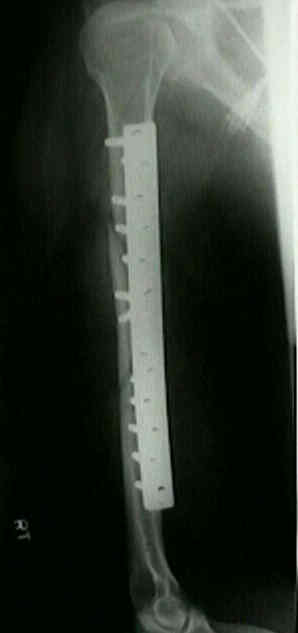
- with plate fixation of the humerus, the anterior approach is preferred for proximal and mid-diaphyseal frx
w/ application of plate to anterolateral aspect of the humerus (see humeral shaft fractures);
- interval lies between deltoid and pectoral nerve proximally and involves a brachalis spliting incision distally;
- relative contra-indications:
- fractures w/ distal extension should not be fixed using anterolateral approach since plate will have to be placed on lateral
column which is thin in the saggital plane;
- Position:
- supine position w/ bump under scapula;
- arm is positioned on an arm board;
- w/ proximal shaft fractures, always prep past the shoulder, since the incision may have to be extended on some occassions;
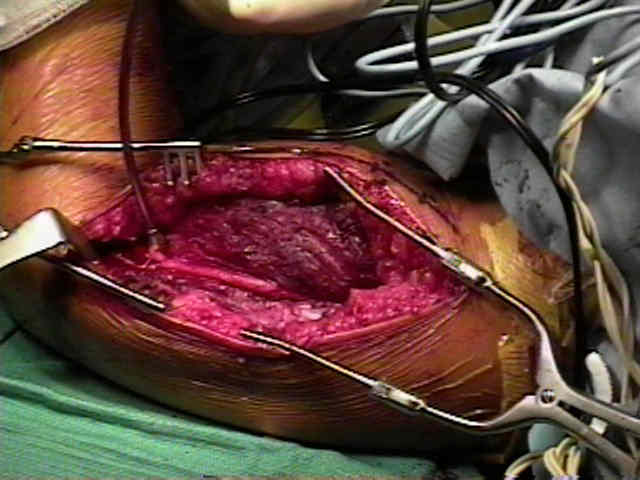
- Surgical Exposure:
- incision follows distal deltopectoral groove to deltoid insertion & then continues along lateral border of biceps, ending at middle
of cubital fossa;
- further proximal exposure is achieved by extending incision and deep dissection along deltopectoral groove (similar
to anterior approach to the shoulder:);
- cephalic vein is retracted medially or laterally;
- tributaries of the cephalic vein converge on it in deltopectoral groove;
- it pierces clavipectoral fascia between pectoralis minor & clavicle, along w/ thoracoacromial vessels & lateral pectoral nerve;
- deltoid detachment:
- w/ proximal humeral frx (just below the neck), more deltoid may have to be stripped from clavicle;
- medial fibers of deltoid are subperiosteally stripped from clavicle, allowing deltoid to be reflected laterally;
- at this point, consider how deltoid will be closed;
- preserve both superficial and deep fascia which invests deltoid muscle;
- each of these fascial envelopes should be opposed to trapezial fascia;
- with a proximal shaft fracture, the deltoid insertion may have to be partially stripped inorder to accomodate plate placement;
- note that the deltoid insertion is broad and therefore it may be partially elevated with no functional consequence;
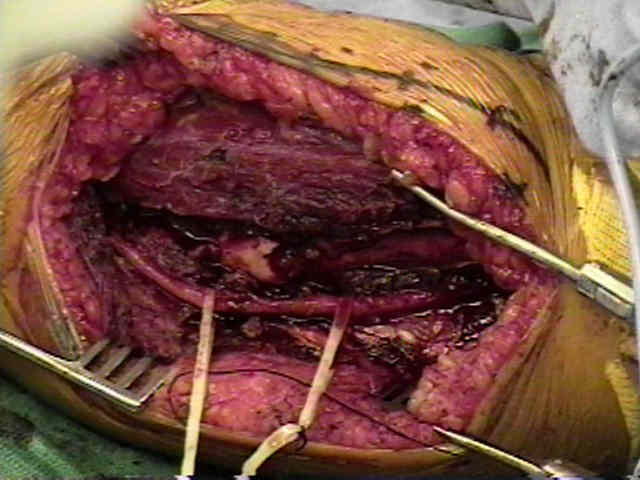
- identification of radial nerve:
- radial nerve lies a few fingerbreadths below and behind the deltoid insertion as it comes forward around the humerus;
- more distally, the radial nerve is identified after radial nerve pierces the lateral intermuscular septum, it can be identified in the
interval between the brachioradialis and brachialis;
- as noted by Gerwin et al, nerve crosses posterior aspect of humerus at 20-21 cm proximal to medial epicondyle and 14-15 cm
proximal to lateral epicondyle;
- ref: Alternative operative exposures of posterior aspect of the humeral diaphysis with reference to the radial nerve.
- alternatively the nerve can be found a distance equal to the length of a 8 hole Synthes DC plate above the olecranon fossa;
- remember than the nerve hugs the posterior surface of the humerus (spiral groove) and that the entire length of nerve around
spiral groove needs to be identified so that retractors are not placed over the nerve;
- when using the anterior approach to plate the humerus, note that the radial nerve is opposed to the posterior surface of the
humerus and may be damaged by drills, taps, and screws;
- with plate fixation, the nerve will generally end up lying on the surface of the plate;
- with humeral fractures across the spiral groove, there is the option of radial nerve transposition;
- ref: Radial nerve transposition with humeral fracture fixation: preliminary results.
- brachialis split:
- at distal edge of incision, origin of brachialis is encountered;
- at this level, the brachialis blends in with the insertion of the deltoid;
- splitting brachialis down its middle allows distal exposure w/o risking injury to the radial nerve which winds around the
humerus laterally;
- this allows exposure as far as the elbow joint;
- flexing the elbow facilitates the exposure;
- remember the brachialis has a dual innervation (musculotaneous portion medially and the radial nerve portion laterally);
- alternatively consider subbrachial approach:
- ref: Subbrachial approach to humeral shaft fractures: new surgical technique and retrospective case series study
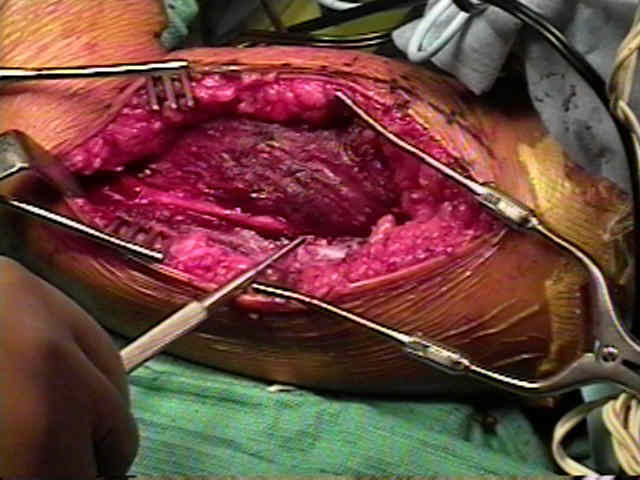
- distal exposure:
- lowest part of front of shaft is approached between brachioradialis which is retracted laterally & brachialis
which is retracted medially;
- more distally, the radial nerve is identified after radial nerve pierces the lateral intermuscular septum, it
can be identified in the interval between the brachioradialis and brachialis;
- lateral cutaneous nerve of forearm emerges at lower lateral border of biceps tendon;
- if the exposure needs to be carried across the elbow joint to the radial shaft, then utilized the anterior approach of henry





Early Results of Bridge Plating of Humerus Diaphyseal Fractures by MIPO Technique.
Lateral approach to the humeral shaft: an alternative approach for fracture treatment.