

- Considerations:
- see plate fixation theory and bone healing with plate fixation;
- candidates for ORIF are humeral shaft frx w/ no comminution w/ enough of an oblique component to allow lag screw fixation;
- in contrast, comminuted transverse fractures may be less satisfying for fixation, and may require bone grafting;
- w/ transverse fractures, lag screw fixation is not possible, and plate prebending may be necessary;
- biomechanical considerations:
- if pt has a stiff elbow, anterior cortex becomes the one under tension;
- in pts with a normal elbow, the posterior cortex is under tension;
- hene, in pts with a mobile elbow, the compression or tension band plates should be applied posteriorly, and in pts
with a stiff elbow, anteriorly;
- Proximal Third Humerus Shaft Frx: (see proximal humerus fracture)
- in upper diaphysis the plate is most commonly placed on the antero-lateral surface of the bone; (see anterior approach)
- in proximal portion of the shaft, where the bone flares to meet the metaphysis, the cortex is thin and very difficult to tap;
- if one inadvertently allows tap to wander, it can easily miss the hole or strip the thread;
- spiral compression plate:
- goal of technique to avoid deltoid muscle stripping by twisting and contouring plate along the proximo-lateral humerus and
along distal-anterior aspect of the humerus;
- authors recommend using a skeletal template to contour the plate prior to surgery;
- proximally the plate is applied on the lateral surface of the greater tuberosity, and more distally the plate crosses anteriorly
between the pectoralis major and the deltoid insertion and ends up lying on the anteiror surface of the humeral shaft;
- the contour of the proximal aspect of the plate misses the bicipital groove (by coursing lateral to it);
- ref: The spiral compression plate for proximal humeral shaft non union: a case report and description of a new technique.
- Mid Humeral Shaft Frx:
- plate selection: (Synthes Humeral Shaft Implants)
- because of large rotational forces placed on humerus, it is best to use a broad 4.5 DCP or LC-DCP w/ staggered screw holes;
- this increases distances between successive screws & decreased likelihood of fissuring the bone longitudinally;
- broad plate allows better rotational stability, 8 cortices allows more rotational stability than 6, and 4.5 mm screws
more than 3.5 mm;
- use of standard 4.5 plate is less optimal for resisting these forces;
- in oblique frxs, 4.5 mm cortex screws can be inserted first as lag screws outside of the plate or thru the plate;
- references:
- Crutch wt bearing on comminuted humeral shaft frx: a comparison of large vs small frag fixation for humeral shaft frx.
- Locked plate fixation of osteoporotic humeral shaft fractures: are two locking screws per segment enough?
- plate position:
- posterior approach:
- generally, frxs of the mid-shaft and distal humerus should be placed posteriorly;
- radial nerve:
- careful to avoid injury to the radial nerve;
- Gerwin M, et al, nerve crosses posterior aspect of humerus at 20-21 cm proximal to medial epicondyle and 14-15 cm
proximal to lateral epicondyle;
- nerve can be found a distance equal to the length of a 8 hole Synthes DC plate above the olecranon fossa;
- with plate fixation, the nerve will generally end up lying on the surface of the plate;
- document the exact spot where the nerve crosses the plate in the operative note;
- with humeral fractures across the spiral groove, there is the option of radial nerve transposition;
- transposition of the radial nerve:
- references:
- Alternative Operative Exposures of Posterior Aspect of the Humeral Diaphysis with Reference to Radial Nerve
- frx reduction:
- lag screw insertion is the easiest technique to achieve reduction;
- noting the significant amount of torque with ADLs, every attempt to insert as many lag screws as possible, including
lag screw fixation of butterfly fragments;
- if necessary lag screws can be countersunk to allow the plate to be applied over the lag screws;
- w/ frx comminution consider need for BMP patch or consider frx shortening (inorder to maximize cortical
opposition);
- plate application:
- distal humerus flares in coronal plane, allowing easy application of broad 4.5 plate over the posterior humeral surface;
- broad plate allows rotational stability, 8 cortices allows more rotational stability than 6, and 4.5 mm screws
more than 3.5 mm;
- posterior position of the radial nerve is almost exactly the distance of a 8 hole DCP plate from the olecranon fossa;
- with distal fractures, consider using an 8 hole plate (with the nerve positioned immediately above the plate);
- with shaft fractures, use a 10-12 hole plate, with no screws applied where the radial nerve crosses the plate;
- dyanmic compression: original concept of non locking dynamic compression is far more important than insertion of
non compressed locking screws;
- humeral fractures treated with plates need as much dynamic compression as possible;
- prebending may not be necessary because of the humeral curvature flares at either end of the bone, will often keep the
center of plate off of the near cortex (already prebent)
- locking screws are for the ends of the plate only (for torsional stability);
- references:
- Locked plate fixation of osteoporotic humeral shaft fractures: are two locking screws per segment enough?
- anterior approach:
- some surgeons, however, favor anterior approach for mid-shaft frx inorder to avoid injury to radial nerve which lies in
posteriorly in spiral groove;
- inorder to achieve fixation w/ 4 screws above the frx, the plate will often have to come to rest underneath of radial nerve;
- hence, anterior approach is generally favored for humeral fractures of proximal and mid diaphysis w/ plate applied to
anterolateral surface of humerus;
- in the saggital plane the distal humerus narrows, and therefore, application of the broad plate over the anterolateral surface
may be difficult (note that 4 screws must be inserted distal to the fracture);
- with insertion of narrow plate, attempt to insert screws in a divergent direction inorder to "stagger" the screws;
- examples:

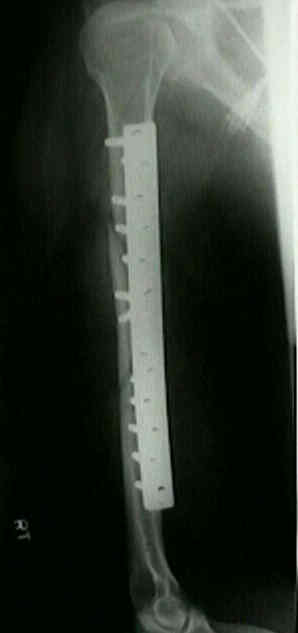

 ***
*** 


- Distal Humerus:
- frxs of distal 2/3 of the humeral shaft should be placed posteriorly (see posterior approach to humerus);
- 4.5 DCP;
- 3.5 mm DC plates should be used only in the supracondylar area;
- two 3.5 mm recon plates extending down supracondylar ridges gives good purchase on short distal fragment;
- ref: Tips and Techniques- Surgical Fixation of Extra-articular Distal Humerus Fractures with a Posterolateral Locking
Compression Plate (LCP).
- example:
- Complications:
- non-union: approximately 5%;
- infection: most often occuring in open fractures
Open reduction and internal fixation of humeral shaft fractures. Results using AO plating techniques.
Plate fixation of the humeral shaft for acute fractures, with and without radial nerve injuries.
[The treatment of humeral shaft fractures. Results of a prospective AO multicenter study].