

 - See:
- See: - Innervation
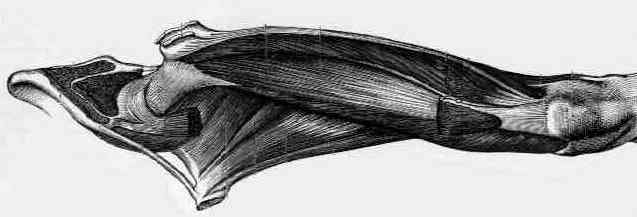
- Rectus Femoris / Intermedius / Lateralis / Medialis
- Extensor Mechanism Injuries of the Knee
- Rupture of the Quadriceps
- Rectus Femoris:
origin:
- straight head: anterior inferior iliac spine
- reflected head: groove on upper brim of acetabulum;
insertion: upper border of patella by the ligamentum patella into tibia tuberosity;
reversed origin-insertion action: flexes the pelvis on the femur and gives anterior stabilization to the pelvis;
nerve supply: femoral, L2, L3, L4; (see innervation)
synergists: psoas, sartorius, tensor fascia lata, vastus lateralis, vastus medialis, vastus intermedius;
arterial supply: ascending branch of LFCA
- ref: Contribution of rectus femoris and vasti to knee extension. An electromyographic study.
- Vastus Intermedius:
origin: proximal 2/3 of the anterolateral surface of the femur, lower 1/2 of the linea aspera, upper part of the lateral supracondylar line; lateral intermuscular septum;
insertion: by tendons of the rectus and vastus muscles into the superior border of the patella and by the ligamentum patella into the tibial tuberosity;
action: extends the leg at the knee;
nerve supply: femoral, L2, L3, L4; (See innervation)
synergists: rectus femoris, vastus medialis, vastus lateralis;
arterial supply: descending branch of LFCA;
- Vastus Lateralis:
origin: upper part of intertrochanteric line, anterior and lower borders of greater trochanter, lateral lip of gluteal tuberosity, upper half of linea aspera, lateral intermuscular septum, and tendon of maximus;
insertion: lateral border of the patella by the ligamentum patella into the tibia tubercle;
action: extends the leg at the knee and draws the patella laterally;
nerve supply: femoral, L3 > L2, L4; (see innervation)
synergists: rectus femoris, vastus intermedius, vastus medialis;
arterial supply: descending and transverse brs. of LFCA;
- Vastus Medialis:
origin: lower 1/2 of the intertrochanteric lines, medial lip of linea aspera, upper part of medial supracondylar line, medial intermuscular septum tendons of adductor magnus and adductor longus;
insertion: Medial border of the patella by the ligamentum patella into the tibia tuberosity; 
action: extends the leg at the knee and draws the patella medially;
nerve Supply: femoral, L3 > L2, L4; (See innervation)
synergists: rectus femoris, vastus lateralis, vastus intermedius
- Gait Characteristics:
- at normal walking speeds the limb behaves as pendulum, w/ near full extension of the knee joint as it preparare for heel-strike;
- during the first 5% of the gait cycle, the quadcrips generate peak intensity of 25%;
- after the first 20% of the gait cycle, the quadriceps become silent;
- exam:
- note that normally an examiner will not be able to "break" a quadriceps unless it is severely weakened;
- 4/5 strength will have 40% of normal strength;
- note that even w/ +3 stength, gait will be relatively normal;
- Quad Paralysis:
- when quadriceps muscle is paralyzed, walking on level surface may appear to be entirely normal;
- at full extension, action of the quadriceps is not necessary for stability of knee joint; if the line of gravity is maintained anterior to the axis of motion of the knee joint, full extension persists through the stance phase;
- w/ quad paralysis, however, the patient will be unable to run and may have difficulty with stairs, because in these cases, full extension is not attained and the knee tends to buckle into flexion;
- patients will often walk with the leg externally rotated inorder to help "lock" the knee at heel strike;
- associated conditions:
- in the case of a weak quadriceps and triceps, the occurance of an equinus contracture or a hinged AFO w/ dorsiflexion block will both prevent excessive knee flexion (buckling) and excessive ankle dorsiflexion during stance phase;
- hence, in this case the equinus contracture is beneficial;
- management:
- when this muscle is quite weak, a long leg brace may be needed to support knee joint in full extension, inorder to prevent knee from buckling during gait;
- consider adding a cushioned heel to the patient's shoe inorder to provide additional knee stability at heel-strike heel strike;
- Quadriceps Contussion:
- Quadriceps contussions: West Point update.
- Quadriceps contusions: clinical results of immediate immobilization in 120 degrees of knee flexion.
Coactivation of the hamstrings and quadriceps during extension of the knee.
A study of quadriceps excursion, torque, and the effect of patellectomy on cadaver knees.
Ruptures of the extensor mechanism of the knee joint.
Relationship Between Hypovascular Zones and Patterns of Ruptures of the Quadriceps Tendon
Injection fibrosis in the quadriceps femoris muscle in children.
Quadriceps myofibrosis. A complication of intramuscular injections.