- Biomechanics of Screw-Plate Angle
- Checklist
- Sliding Hip Screw w/ Unstable Frx
- High Angle Plates
- Low Plate Angle
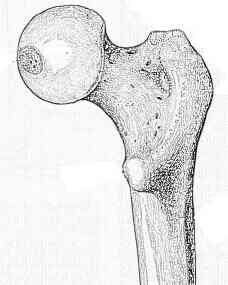
- Nail Placement in Femoral Head and Neck
- Screw Length
- Sliding Screw Fixation in Femoral Neck Frx
- Sliding Screw Fixation in Subtroch Frx
- Discussion: Indications and Contraindications:
- pre op planning:
- note whether lesser troch is fractured, and whether there is posteromedial comminution (ie. is frx is stable or unstable);
- this determines whether sliding screw can be inserted using standard techniques versus the need for osteotomy (Sarmento, Dimon, or Wayne);
- note that most surgeons will attempt to a achieve a stable anatomic reduction over a stable non-anatomic reduction (as occurs the osteotomies);
- ref: How effective are osteotomies for unstable intertrochanteric fractures?
- cautions and contraindications:
- lateral wall comminution (indicates reverse obliquity fractures or transtrochanteric fractures)
- reverse obliquity and low intertrochanteric fractures:
- in reverse obliquity frx, starndard sliding screw technique may cause distraction at frx site (rather than compression) and may cause excessive medialization of femoral shaft in relation to femoral neck (lateralization of proximal femoral fragment);
- Technique:
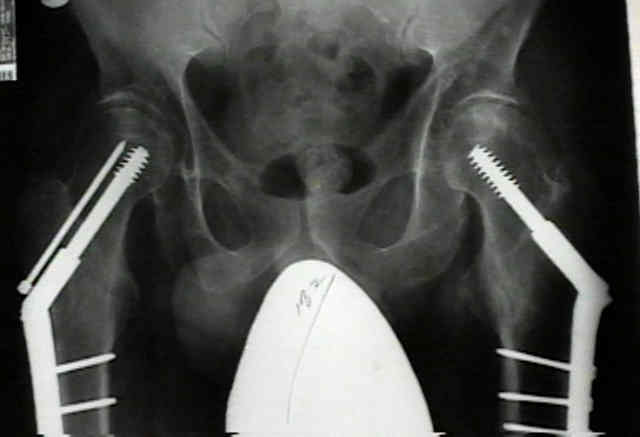
- patient is positioned on frx table in standard fashion;
- Reduction Technique:
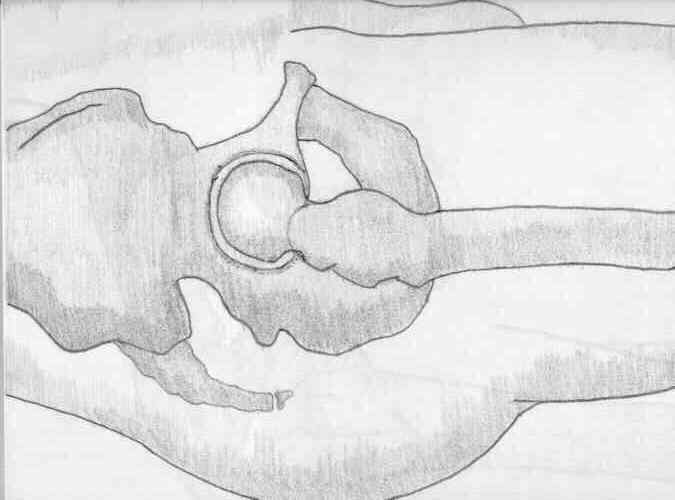
- note that it is necessary to obtain a closed reduction under flouro prior to making the incision, to ensure that all aspects of the fracture can be visualized, including the femoral head on both the AP and lateral views;
- once fracture is reduced, use flouro to help determine the amount of femoral neck anteversion;
- if a true lateral view is obtained, angulation of the flouroscope above the horizontal will indicate the amount of anterversion (and direction of guide pin);
- ref: Sliding characteristics of compression hip screws in the intertrochanteric fracture: a clinical study.
- Screw-Plate Angle
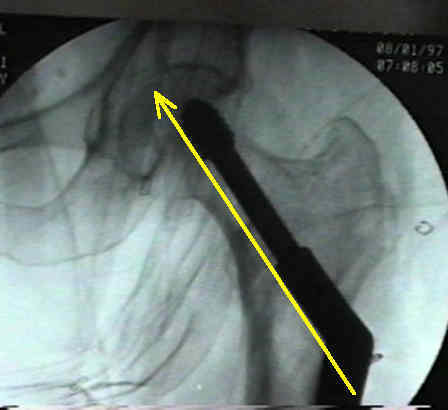
- Guide Pin Placement and Depth and Screw Length
- Reaming and Lag Screw Insertion
- Plate Length:
- in osteoporotic bone, up to six screws (12 cortices) may be necessary;
- in a prospective study by Bolhofner, et al. (1999), a 2 hole sliding screw plate was used in 70 consecutive patients w/ intertroch frx;
- there were three hardware failures, but none of these occured due to loss of fixation of the two hole side plate;
- the authors noted a relatively short operative time and low blood loss;
- references:
- Results of intertrochanteric femur fracture treated with a 135-degree sliding screw with a two-hole side plate.
- Optimal side plate fixation for unstable intertrochanteric hip fractures.
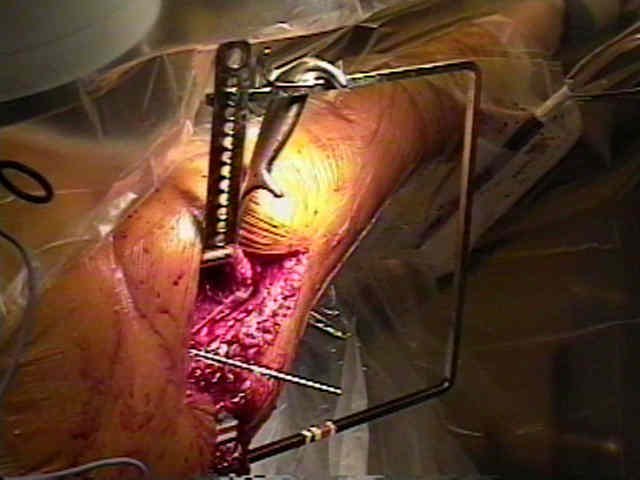
- Plate Application:
- Medial Fragments:
- medial fragments may be secured w/ lag-screw tech if they can be captured w/o extensive dissection or periosteal stripping.
- biomechanical studies have shown increased stability of frx after fixation of large medial fragments;
- grafting of medial defects w/ autogenous bone should be done to promote early healing if medial comminution is present.
- reference:
Screw fixation of the lesser trochanteric fragment.

- Compression at Frx Site:
- although sliding hip screw allows postop impaction at frx site, it is essential to obtain impacted reduction at time of surgery;
- this impacted position avoids excessive postop collapse that may exceed sliding capacity of the device;
- release traction, and insert compression screw;
- if a short barrel has been used or if a screw has been inserted 0.5 to 1 cm past the standard depth, then compression screw should be retained;
- remember, however, that the compression screw may become prominent and cause symptoms;
- Wound Closure:
- remember that most of these patients will require postoperative DVT prophylaxis, and therefore a tight wound closure is essential;
- references: Why use drains?
- Post Operative Care:
- forces acting on the hip joint
- as noted by Koval KJ et al (1998), elderly patients who are allowed to bear wt as tolerated, will voluntarily limit loading of the injured limb;
- during the first postoperative week patients load the injured limb about 50% as compared to the uninjured limb, and by 12 weeks the injured limb was loaded 87%;
- reference:
- Postoperative weight bearing after a fracture of the femoral neck or an intertrochanteric fracture.
- Controversies:
- rheumatoid arthritis
- over one third of patients w/ RA treated w/ a sliding hip screw (for intertroch frx) will sustain a major complication (AVN, nonunion, loss of fixation);
- w/ significant joint arthrosis, total hip arthroplasty may be indicated in some cases;
- reference:
- Intertrochanteric fractures of the femur in rheumatoid arthtitis patients.
- basilar neck frx
- Complications:
- Varus Collapse w/ Screw Cut Out:
- more common w/ high angle plates (150 deg);
- Avascular Necrosis:
- Avascular necrosis of the femoral head after intertrochanteric fractures.
Three cancellous bone screws versus a screw-angle plate in the treatment of Garden I and II fractures of the femoral neck.
Internal fixation of femoral neck fractures. Two methods compared.
A biomechanical analysis of the sliding hip screw: the question of plate angle.
Current approaches to experimental bone grafting.
Compression screw fixation for displaced subcapital fracture of the femur. Success or failure
Biomechanical analysis of the sliding characteristics of compression hip screws.
Treatment of femoral neck fractures with the sliding compression screw.
Trochanteric fractures: Influence of reduction and implant position on impaction and complications.