


- See: Unstable Intertrochanteric Fractures
- Discussion:
- in reverse oblique fractures, the major frx line extends from proximal-medial to distal-lateral through intertroch-subtrochanteric region;
- marked tendency toward medial dispacement of shaft 2nd hip adductors;
- tendency for medial shaft migration may result in penetration of internal fixation device into the joint;
- comminution of greater troch & adjacent posterolateral shaft of femur also predisposes to such medial shaft migration;
- cautions with sliding screw fixation: in contrast to stable intertrochanteric fractures, sliding screw fixation may cause reverse obliquity fractures to distract (rather than compress), resulting in extensive medialization of the shaft and poor frx healing;
- Treatment: Piriformis Fossa Disrupted:
- the subtrochanteric portion of this fracture needs to be first reduced with a bone reduction clamp, followed by either lag screws or cerclage wires;
- this type of frx is fixed in manner similar to that used for Type-IV frx, however, reduction may be difficult, because adductors & iliopsoas are intact & will tend to pull distal fragment medially while proximal fragment is abducted, flexed, & pulled laterally;
- if the reverse obliquity fragment is especialy long or if there is additional subtrochanteric comminution, then consider placing the patient in the lateral position (rather than supine on the frx table) since this keeps the leg free to facilitate the reduction and facilitates posterior femoral exposure which may be required inorder to affect a direct reduction;
- if the lateral position is used, then the surgeon must estimate the proper sliding screw anteversion by placing his finger along the anterior surface of the femoral neck;
- once the guide pin is inserted, the tight must then be placed in the frog leg lateral position (full external rotation) in order to achieve a frog leg lateral, and the anteversion of the guide pin can be judged;
- if the fracture books open in the frog leg lateral position, then several guide pins can be inserted to prevent this;
- these frx need to be fixed w/ screw-plate placed at lower angle (95 deg) so that fixation device does not have to be placed directly, along frx site;
- lower plate angles also allow the sliding lag screw to be placed more proximally, and therefore either one or two cortical screws can be placed above the frx site;
- w/ oblique fractures it is optimal to place one or two screws as lag screws across the frx site;
- see: sliding screw fixation of subtrochanteric fractures and 95 deg screw fixation;


- Treatment: Piriformis Fossa Intact:
- may be treated like a subtrochanteric fracture (IM nailing for subtrochanteric fractures)
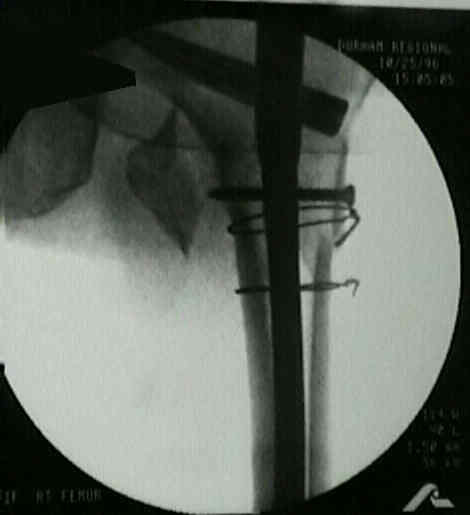
- if the piriformis fossa is intact, then the frx is amenable to reduction w/ cerclage wires, and subsequent fixation w/ a Synthes IM Nail w/ spiral blade plate;
- it is essential that a proximal interlocking screw be inserted, inorder to achieve two points of fixation proximal to the fracture;
- in the report by Sadowski C, et al (2002), the authors compared the results of intramedullary fixation with those
of plate fixation for reverse intertrochanteric fractures in elderly patients;
- patients treated with an intramedullary nail had shorter operative times, fewer blood transfusions, and shorter hospital stays
compared with those treated with a 95° screw-plate;
- implant failure and/or nonunion was noted in seven of the nineteen patients who had been treated with the 95° screw-plate;
- only one of the twenty fractures that had been treated with an intramedullary nail did not heal;
- ref: Treatment of Reverse Oblique and Transverse Intertrochanteric Fractures with Use of an Intramedullary Nail or a 95° Screw-Plate. A Prospective, Randomized Study



Treatment of Reverse Oblique and Transverse Intertrochanteric Fractures with Use of an Intramedullary Nail or a 95° Screw-Plate. A Prospective, Randomized Study
Reverse Obliquity Fractures of the Intertrochanteric Region of the Femur.