- Incision:
- although the closed reduction may require external rotation of the hip, the initial incision is facilitated w/ slight internal rotation of the leg;
- make straight lateral incision two finger breadths below the vastus ridge to a point 5-7 cm distally;
- typically the incision is made too cephalad, and typically is made much longer than is necessary;
- large Bechman Retractors may be used to retract the subQ tissue in obese patients;
- Ilio-Tibial Band:
- a periosteal elevator is used to sweep subQ tisse from either side of IT band;
- incise fascia lata in line w/ the incision;
- best performed by making a small nick w/ a knife, and completeing the incision w/ Mayo scissors;
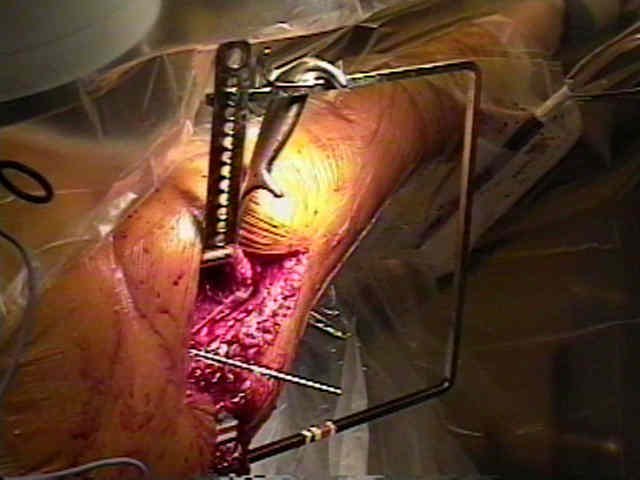
- Rectraction:
- if surgical assistants are not available, consider applying a Charnley retractor deep to the IT band (or large self retaining retractors);

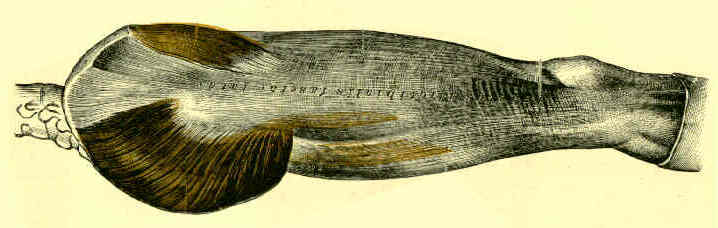
- Vastus Lateralis Incision:
- bluntly sweep away the adhesions between the vastus lateralis and the IT band;
- retract the vastus lateralis anteriorly using either the surgeon's hand or large Hibbs type Retractors, inorder to place the muscle undertension;
- alternatively the vastus can be shifting anteriorly, by clamping two Kochers into the posterior vastus fascia, and then pushing the Kochers anteriorly and medially so that they come to rest on the anterior femoral surface;
- use a periosteal elevator too bluntly split the posterior 20% of the vastus directly down to bone, and then elevate it off the bone;
- remember that at the superior aspect of the incision, only a small amount of the muscle requires elevation (avoiding excessive stripping will decrease postop pain and will facilitate rehabilitation;
- in cases of an especially complicated frx which cannot be closed reduced, then a more extensive exposure is required;
- use cautery to make a "L" shaped incision across the vastus origin, which starts along the vastus ridge until its posterior edge is reached, and then continue the incision distally for about 5 cm along the posterior tendinous border of the vastus;
- before a more distal dissection is made, elevate the "L" shaped musculotendinous flap (previously made) subperiosteally from the femur (first using cautery and then a periosteal elevator);
- subsequently incise along the posterior tendinous border of the vastus lateralis for a few additional centimeters;
- excessive muscular dissection is not necessary and only stirs up bleeding;
- in this case, one or possibly two perforating vessels may become visible as they are traveling from posterior to anterior to supply the vastus;
- these vessels should be carefully cauterized since a constant ooze from these vessles may not be obvious after triple remear has been inserted;
- incising over the vastus ridge frees the vatus tendon and allows the muscle to be retracted anteriorly and distally; (which will allow the plate to be slid underneath the retracted muscle);
- insert 2 large Bennet retractors over the anterior edge of the femur, and rest the retractor handles underneath the previously applied Charnely retractor;
- use a periosteal elevator to strip the remaining tissue from the lateral aspect of the femur