

- See:
- High Angle Plates
- Low Plate Angle
- Nail Placement in Femoral Head and Neck
- Screw Length
- Unstable Intertrochanteric Fractures
- Discussion:
- sliding device w/ screw plate angle closest to combined force vector allows optimum sliding and impaction.
- closer nail-plate angle to resultant vector of forces across hip, more force available to assist impaction;
- plates are available in 5 deg increments from 130-150 deg, however, 135 & 150 deg plate angles are the most commonly used;
- regardless of particular type of device used, it is essential to obtain maximal holdin capacity in the head;
- matching the anatomic neck-shaft angle:
- screw-plate angle may be determined w/ use of variable-angle guide after guide pin has been inserted or it can be chosen from preop radiographs;
- guide pins are inserted at highest angle possible along medial cortex of neck fragment, while still being in center of femoral head on both AP & lateral radiographs;
- as pointed out by Meislin RJ, et al (1990), there is no benefit to proximal medial femoral strain distribution using this method;
- the authors note that most intertrochanteric fractures can be treated successully w/ use of a 135 deg or 140 deg SHS;
- as noted by Den Hartog BD, et al (1991), mean load to failure was signficantly increased in unstable intertrochanteric fractures by re-establishment of medial contact (using an osteotomy, use of a high angle plate, and placement of the lag screw in the center of the femoral head;
- A biomechanical analysis of the sliding hip screw: the question of plate angle.
- Treatment of the unstable intertrochanteric fracture. Effect of the placement of the screw, its angle of insertion, and osteotomy.
- low plate angle:
- 135 deg plates are indicated for most patients - for anatomic reduction;
- device that is placed at lower angle has less force working parallel to sliding axis & more force working perpendicular to sliding axis;
- this perpendicular force acts to jam or bend the device, thereby preventing impaction.
- device that is placed at lower angle may be used effectively in stable frx because controlled collapse is not important for impaction of the fracture and early weight-bearing;
- high angle plates:
- 150 deg plate angle may rest in weak bone of anterosuperior quadrant of femoral head unless valgus reduction & low nail placement are obtained;
- nails in superior aspect of the femoral head can inadvertently interrupt lateral epiphyseal vessels that supply most of blood to femoral head;
- technically, surgeon cannot place sliding device at high angle in small hip or in hip w/ varus deformity.
- mechanically, it is desirable to place sliding device at as high angle as clinically possible while still maintaining placement of device in the center of head;
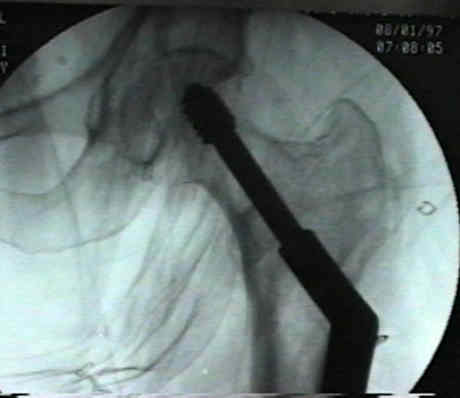
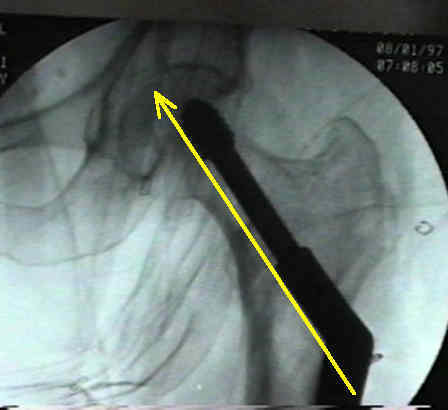
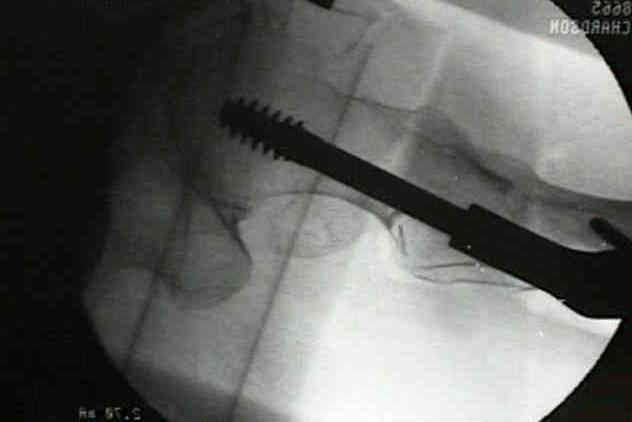
- Case Example:
- this patient's fracture healed, but it probably would have been better to position the screw more inferiorly than was done in this case;



A biomechanical analysis of the sliding hip screw: the question of plate angle.
Trochanteric fractures: Influence of reduction and implant position on impaction and complications.