

- See:
Watson Jones Approach
Smith Peterson Approach
- Discussion:
- in direct lateral approach, a curvilear split is made thru the anterior portion of the gluteus medius and vatus muscles, in order to gain access to the anterior face of the hip joint;
- this approach allows a rather direct approach to the hip with minimal need for surgical assistants and affords excellent acetabular exposure;
- indications:
- alcoholism:
- dislocations may occur in upto 20% of alcoholics who undergo THR via a posterior approach;
- consider the Hardinge approach for any patient who will have difficulty with complying with the usual hip precautions following surgery;
- significant hip flexion contracture:
- consider the Hardinge approach for patients w/ significant contracture;
- note that many patients will have a reduced hip flexion contracture under anesthesia, which will give the surgeon the false sense of having corrected the contracture;
- unfortunately, many of these patients will re-gain their flexion contracture postoperatively;
- if the surgeon attempts to correct the contracture by performing an aggressive anterior capsulotomy, then there is an increased risk of dislocating out the front; 
- PreOp:
- Checklist for THR
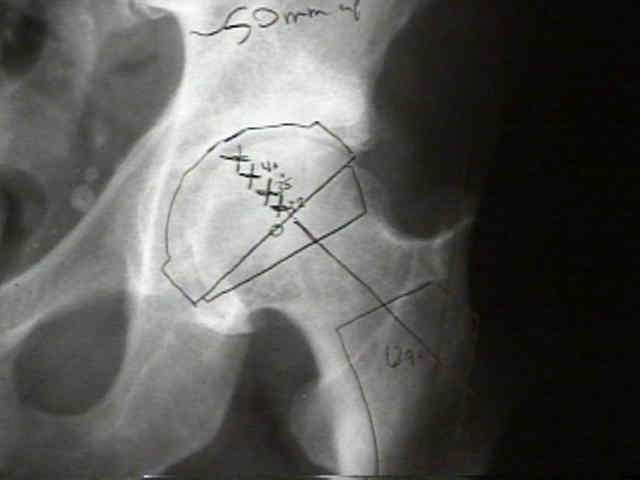
- Radiographs
- Positioning:
- lateral position, with a sterile surgical drape folded in a "saddle bag" fashion to allow the leg to hang over the edge of the table in a flexed and externally rotated position (inside of the saddle bag);
- ensure that the sterile drapes are tied together underneath the operating room table (by the unscrubbed assistant) so that the drapes do not slide off the table as the leg is placed in the saddle bag;
- Incision:
- patient lies in a straight lateral position;
- skin incision is actually similar to that of the posterolateral approach, except that the incsion needs to be shifted anteriorly a few cm; in order to center the exposure over the anterior femoral neck when it is fully externally rotated;
- the reason for this becomes evident once the femur is prepared for reaming;
- to ream and broach the femoral canal, the leg is flexed and externally rotated so that the leg hangs off the side of the bed;
- reaming is performed from proximal-posterior to distal anterior, and therefore the broach handle will lie in the middle of the posterior skin incision;
- Deep Dissection:
- tensor fascia:
- distally the tensor fasciae latae is split in line with the femur;
- proximally the split should curve slightly anteriorly towards the ASIS;
- clear off adhesions from the under-surface of the tensor fasia, and insert a Charnley retrator, so that the greater trochanter is in the center;
- elevate and peel the trochanteric bursa posteriorly so that the distal medius and the proximal lateralis are clearly defined;
- medius incision:
- note the crescent shaped course of the vastus medialis, with the anterior fibers of the medius lying in a horizontal position;
- spliting the most anterior fibers of the medius provides good exposure and is less likely to deinnervate the medius;
- take care not to injure the minimus muscle;
- place a tagging suture 5 cm above the greater trochanter;
- note that the superior gluteal nerve enters posterior surface of this muscle and is at risk for injury (if dissection is carried too far proximally);
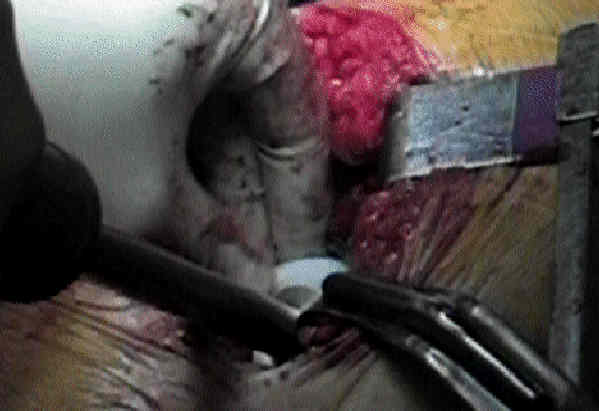
- starting at the vastus ridge of the greater trochanter, use caurtery to incise proximally along the anterior 1/3 of the greater trochanter and continue more proximally by splitting the medius tendon upto the tagging suture;
- sometimes the gluteal nerve can be felt along the undersurface of the medius;
- alternatively, use a sharp wide osteotome to take a 3-4 mm thick silver of the anterolateral trochanter and trochanteric ridge (which will contain both the minimus and vastus lateralis);
- ref: Partial anterior trochanteric osteotomy in total hip arthroplasty: Surgical technique and preliminary results of 127 cases
- vastus lateralis incision:
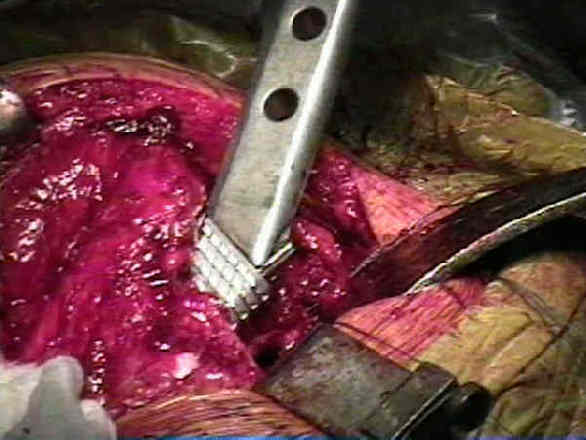
- beginning at the vastus ridge at the point of the medius incision, use cautery to incise through the vastus lateralis tendon and muscle in line with its fibers;
- minimus and capsular incision:
- at this point in procedure, the hip partially flexed and fully externally rotated inorder to rotate the femoral neck into full profile;
- the posterior 2/3 of the vastus and the medius are left undisturbed;
- deep to the gluteus medius lies the minimus, whose fibers should also be split in line with their fibers along w/ the underlying capsule;
- the minimus fibers tend to run north to south;
- use cautery to mobilize the anterior portions of the medius, minimus and lateralis off their attachements to the anterior greater trochanter, all the
- during the dissection, it is essential to keep the medius and vastus lateralis attached together as one flap, inorder to facilitate wound closure;
- once the dissection, proceeds down to the anterior intertrochanteric line, flex and externally rotate the hip, so that the leg is swung forward over the table, with the leg lying inside the sterile "saddle bag;"
- this causes the anterior portion of the medius to swing forward;
- at the intertrochanteric line, the tendinous insertion of the gluteus minimus may be encountered, and is elevated off w/ cautery;
- the dissection procedes down to the anterior face of the hip capsule;
- the hip capsule is identified and incised w/ an inverted "T" incision;
- Hip Dislocation and Acetabular Exposure:
- in the case of femoral neck fracture, acetabular exposure is optimized by extending the leg, which allows the proximal femur to be retracted posteriorly;
- a slightly low femoral neck resection will help strip off the posterior capsule, which facilitates removal of the femoral head;
- in the case of a total hip replacement, the hip is dislocated by flexing and externally rotating the hip, (so that the leg is swung forward over the table, with the leg lying inside the sterile "saddle bag");
- Femoral Neck Resection
- Acetabulum:
- Acetabular Exposure and Preparation for Reaming:

- Acetabular Reaming:
- Acetabular Cup Insertion:
- acetabular cup position:
- screw insertion:
- some surgeons delay insertion of acetabular screws until, a trial reduction has been carried out, so that the cup position can be changed if needed;
- this is an especially prudent consideration if an anterior capsulotomy has been performed;
- Femoral Component:

- Entry into Femoral Medullary Canal
- Femoral Reaming:
- care is taken to maintain 15-20 deg of anteversion;
- references: Femoral anteversion and restricted range of motion in total hip prostheses.
- Femoral Broaching
- Trial Reduction:
- prior to reducing the hip, ensure that the center of the femoral head is approximately at the level of the greater trochanter;
- once trial reduction has been completed, the trial acetabular liner is removed, the remaining acetabular dome screws are inserted (if they have not been already) and the definitive liner is inserted;
- the sciatic nerve should be palpated w/ the hip in flexion (and leg extened) to ensure that the nerve is not under excessive tension (especially if the leg has been lengthened);
- Insertion of Cementless Femoral Stem
- Insertion of Cemented Femoral Stem
- cementing: preparation and technique
- Final Trial:
- prior to applying the femoral head, consider applying a trial head to be sure that stability is optimal;
- note that if a Steinman pin as been used to retract the medius, it should be removed at this point, since it may placed signficant tension on the medius and give a false sense of hip stability;
- Wound Closure:
- deep layer: includes hip capsule and gluteus minimus;
- gluteus medius and vastus lateralis;
- tensor fascia;
- Cautions:
- superior gluteal nerve enters posterior surface of this muscle and is at risk for injury (if dissection is carried too far proximally);
- residual abductor weakness and limp may occur post op if there is an avulsion of the repaired of anterior portion of abductors;
- consider removal of anterior portion of abductors w/ attached thin wafer of bone from anterior edge of greater trochanter to facilitate later repair;
- abductor function is better following bony reattachment of the anterior portions of these muscles
The direct lateral approach to the hip.
Damage to the superior gluteal nerve after the Hardinge approach to the hip.
The direct lateral approach to the hip for arthroplasty. Advantages and complications.
Translateral surgical approach to the hip. The abductor muscle "split".
Comparison of heterotopic bone after anterolateral, transtrochanteric, and posterior approaches for total hip arthroplasty.
The trochanteric approach to the hip for prosthetic replacement.
Exposure of the hip using a modified anterolateral approach.
Exposure of the hip by anterior osteotomy of the greater trochanter. A modified anterolateral approach.
Abductor function after total hip replacement. An EMG and clinical review.
Dislocation after total hip arthroplasty using the anterolateral abductor split approach.
Partial anterior trochanteric osteotomy in total hip arthroplasty: Surgical technique and preliminary results of 127 cases