

 - See: Total Hip Replacement Menu:
- See: Total Hip Replacement Menu: - acetabular components
- acetabular component position:
- Discussion:
- occurs in 1-4% of primary THA and upto 16% in revision cases;
- about 74% of THR dislocations are posterior, 16% anterior, and 8% lateral; (from
Cobb TK, et al. (1996));
- most commonly caused by looseness of hip (improper neck length), and component malposition
(see acetabular component position);
- note the association of prior spine fusion with THR dislocation:
- Abnormally High Dislocation Rates of Total Hip Arthroplasty After Spinal Deformity Surgery
- Prosthetic Dislocation and Revision After Primary Total Hip Arthroplasty in Lumbar Fusion Patients: A Propensity Score Matched-Pair Analysis.
- revision arthroplasty:
- dislocation is much more common in revision THA;
- careful testing w/ trial components w/ correction of neck lengths w/ correction of neck length, impingement, & repair of
trochanter may avoid this complication;
- ref: The elevated-rim acetabular liner in total hip arthroplasty: relationship to postoperative dislocation.
- Differential Dx:
- patient risk factors:
- excessive alcohol intake (dislocation of up to 20%);
- in patients w/ DDH, risk of dislocation may be as high as 8%;
- positional dislocations:
- components are positioned correctly & soft tissues are balanced;
- patient puts the hip into a position that is beyond the range possible w/ prosthetic components;
- soft tisse laxity:
- shortening in either verticle or horizontal direction causes soft tissue imbalance, possibly resulting in dislocation;
- radiographs should be evaluated for limb length inequaility;
- late dislocation may be related to gradual stretching of pseudocapsule;
- laxity of soft tissue is most frequent cause of instability of THR when radiographs reveal good position of components; 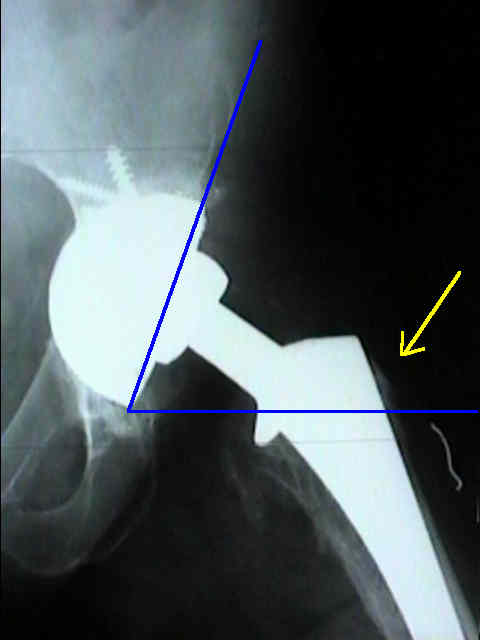
- trochanteric non union is another risk factor for dislocation because of soft tissue tension;
- component malposition: (acetabular component position)
- safe position: 35 +/- 10 deg anteversion 40 +/- 10 deg abduction
- acetabular abduction angle
- horizontal cup placement (less than 40 deg) may lead to early impingement in flexion;
- in this case there is impingement between neck and poly liner;
- result can cause osteolysis, liner dislodgement, and component loosening;
- version of acetabulum (true lateral view) (see radiographic evaluation)
- anteversion is determination directly by measuring angle between line drawn thru axis of metal
shell or wire marker & verticle on cross table lateral view of acetabulum;
- unnoticed forward rotation of pelvis when surgical procedure is done in lateral postion is one cause
of malalignment of component that can result in an unnoticed retroversion position of cup;
- version of femoral component;
- references:
- Factors predisposing to dislocation after primary total hip arthroplasty: a multivariate analysis.
- The effect of orientation of acetabular and femoral components on range of motion of hip at different head-neck ratios.
- Joint motion and surface contact area related to component position in total hip arthroplasty.
- Computed tomographic evaluation of component position on dislocation after total hip arthroplasty.
- Position, orientation and component interaction in dislocation of the total hip prosthesis.
- What Safe Zone? The Vast Majority of Dislocated THAs Are Within Safe Zone for Acetabular Component Position.
- componenet impingement:
- posterior dislocation may be caused by anterior osteophytes which protrude beyond the edge of the acetabular cup;
- anterior dislocation may be partially due to the presence of a high wall liner placed posteriorly;
- overmedialization of the cup:
- more common in protrusio
- overmedialization causes impingement of the femoral neck on the pelvis
- management of this situation may involve use of a lateralized liner (high wall liner will not help this);
- horizontal cup placement (less than 40 deg) may lead to early impingement in flexion;
- in this case there is impingement between neck and poly liner;
- result can cause osteolysis, liner dislodgement, and component loosening;
- acetabular occupancy:
- cause of dislocation in RR, & once hip is rereduced, hip is stable;
- femoral head size:
- component subsidence:
- limb length shortening is a known cause of dislocation;
- lateral / medial offset:
- lateralized femoral stem may be used to restore stability, but this may increase component micromotion;
- ref: Micromotion measurements with hip center and modular neck length alterations.
- obesity:
- Obesity is associated with higher complication rates in revision total hip arthroplasty.
- Dislocation rate increases with bariatric surgery before total hip arthroplasty.
- The influence of obesity on primary total hip arthroplasty outcomes: A meta-analysis of prospective cohort studies.
- Increased hip abduction in high body mass index subjects during sit-to-stand
- Morbid obesity may increase dislocation in total hip patients: a biomechanical analysis.
- Total hip replacement in morbidly obese patients with osteoarthritis: results of a prospectively matched study.
- Assessment:
- need to review operative note for specific details about hip stability;
- flouroscopy to determine range of hip stability and to determine whether any of components are loose
(femoral component, acetabular cup, and acetabular liner);
- exam: neurovascular exam before and after the reduction;

- posterior dislocation
- caused by flexion, adduction, and internal rotation;
- anterior dislocation
- caused by extension, adduction, and external rotation;
- in the example below, the patient sustained an anterior dislocation in the RR;
- it was felt that the dislocation occurred as a result of performing a partial anterior
capsulotomy in addition to the lingering effects of the spinal anesthetic;
- he was placed in a bledsoe brace, which held the hip in 30 deg flexion;


- Reduction Maneuver:
- typically the patient will be placed on a flouro bed (if one is available);
- an assistant stands near the patients head, and provides downward traction on the pelvis;
- the surgeon should step up onto the bed, standing over the patient;
- grasp the patient's leg between the surgeon's arm and armpit, leaving both hands free to grasps the knee;
- surgeon uses his/her legs to effect an appropriate amount of traction, while the surgeon uses his hands to internally and externally
rotate hip (as directed by the flouroscopic picture) inorder to guide the hip into a reduced position;
- difficult reduction:
- ensure that the patient is paralyzed;
- if the femoral head is brought down to the level of the acetabulum and the reduction does not occur, then the femoral head
is most likely posterior, which means that the hip needs to be flexed allowing traction to be directed anteriorly;
- consider placing the patient in the lateral position, allowing flexion, internal rotation and traction in the usual manner;
- references:
- Sciatic Nerve Entanglement Around a Femoral Prosthesis During Closed Reduction of a Dislocated Total Hip Prosthesis:
The Role of Metal-Suppression MRI
- Treatment Options:
- treatment depends on the etiology of the dislocation;
- if alcoholism was related to the dislocation then education and bracing are necessary;
- if component mal-positioning or gluteus medius laxity are present, then these may need to be managed operatively;
- simple closed reduction:
- in general, if more than 2 dislocations have occurred, revision surgery should be considered;
- if a dislocation occurs late after surgery, then consider surgery as recurrent dislocations can be expected;
- references: Late Dislocation After Total Hip Arthroplasty.
- Li E, et al. (2000), the authors followed a total of 1,036 consecutive total hip replacements between 1989 and 1992;
- 40 (3.9%) were known to have dislocated posteriorly (24 of these dislocations occurred after primary replacements,
and 16 after revision);
- 85 % of the dislocations occurred within 2 months and were reduced closed;
- 23 of the 40 dislocated hips (57.5%) redislocated
- 16 of the 40 hips (40%) required reoperation for recurrent dislocation;
- references:
- The Natural History of a Posteriorly Dislocated Total Hip Replacement
- Outcome of treatment for dislocation after primary total hip replacement
- Dislocation of primary total hip arthroplasty and the risk of redislocation.
- trochanteric advancement:
- may be indicated if options for increased neck length are not present;
- revision total hip replacement:
- femoral component revision: increased lateral offset can be achieved by increasing neck length;
- ref: Modular revision for recurrent dislocation of primary or revision total hip arthroplasty.
- acetabular liner:
- as noted by Cobb et al 1996, the presence of a high wall liner can reduce incidence of dislocation in primary THR from
about 3.8% to 2.2%
- the beneficial effect is probably higher w/ revision surgery;
- paradoxically, high wall liner may actually increase incidence of anterior dislocation (due to impingement
between femoral neck and elevated lip of liner);
- liners may also contribute to increased polyethylene wear;
- reference:
- The Elevated Rim Acetabular Liner in Total Hip Arthoplasty: Relationship to Postoperative Dislocation.
- acetabular component revision
- increased anteversion (if posterior dislocation is present);
- increased lateral offset (using lateralized liner);
- constrained acetabular liner component
- bipolar hip arthroplasty as a Salvage Treatment for Instability of the Hip
- in the report by Parvizi J and Morrey BF (2000), reviewed the records of 27 patients who had
undergone bipolar hip arthroplasty as a salvage procedure for the treatment of recurrent instability of the hip after THR;
- all patients had undergone at least two, and a mean of three, stabilizing operative procedures on hip prior to bipolar arthroplasty.
- the mean duration of follow-up was five years (range, two to twelve years), with no patient lost to follow-up;
- bipolar arthroplasty prevented redislocation in twenty-two hips (81%);
- 25 patients (93%) had a stable hip at the time of last followup;
- complications: revision because of disassembly of the cup in one hip, revision bipolar arthroplasty because of continuing
instability in two, resection arthroplasty because of deep infection in two, revision arthroplasty because of recalcitrant groin
pain in one, and revision arthroplasty because of deep infection and superior migration of the implant in one;
- 12 patients in our study had hip pain, and two had severe groin pain;
- refs:
- Bipolar hip arthroplasty as a salvage treatment for instability of the hip.
- Bipolar hip arthroplasty for recurrent dislocation after total hip arthroplasty. A report of three cases.
Dislocation After Revision Total Hip Arthroplasty: an Analysis of Risk Factors and Treatment Options
Hospital Cost of Dislocation After Primary Total Hip Arthroplasty.
Classification and Management of the Unstable Total Hip Arthroplasty