

- Medical Assesment:
- surgical risk assessment
- risk factors for infection: are taken into consideration;
- anesthesia consult and posting
- anesthesia, medical consderations, and timing for femoral neck frx
- autologous blood / cell saver / transamic acid
- preop cardiology, dental, GI, and urological consults
- with history of prostatic hypertrophy or surgery be prepared to have urologist available for foley placement;
- tranexamic acid
- vitamin D:
- Vitamin D deficiency in patients with osteoarthritis undergoing total hip replacement: a cause for concern?
- transfusion considerations:
- preoperative hemoglobin is main indicator for need of postoperative transfusion;
- Hgb less than 11 g/dl is a strong indicator for need for transfusion;
- autologous blood: (see pRBC transfusion)
- 2 units for primary hips) or cell saver;
- disadvantages: time consuming, expense, significant decrease in preop Hbg level (which increases likelihood
of transfusion), possibility of clerical error, possibility of transfusion reaction;
- Sculco TP and Gallina J (1999), 82% of these patients (autologous or PAD patients) required transfusion of their own
blood (vs 50% in patients that did not donate autologous blood), but only 8% of PAD patients required transfusion;
- 34 to 45% of autologous blood was discarded;
- w/ preop Hgb level of less than 11 g/dl about 93-96% of pts required a transfusion vs. only 52-59% of pts w/ preop
Hgb of greater than 14 g/dl;
- w/ THR, expected transfusion requirements are 0.8 units when the Hgb level is more than 14 g/dl vs 1.6 units when
Hgb level is less than 11 g/dl;
- erythropoitin
- references:
- Blood management experience: relationship between autologous blood donatoin and transfusion in orthopedic surgery.
- Efficacy of Intraoperative Blood Collection and Reinfusion in Revision Total Hip Arthroplasty.
- urinary tract
- Are Antibiotics Necessary in Hip Arthroplasty With Asymptomatic Bacteriuria? Seeding Risk With/Without Treatment
- Exam:
- previous incisions:
- limb length: most common cause of apparent limb length inequality is hip flexion contracture;
- vascular status;
- delay surgery if any "minor" infections are present (such as infected ingrown toenail, prostatitis, ect);
- spine:
- Acetabular Anteversion Changes Due to Spinal Deformity Correction: Bridging the Gap Between Hip and Spine Surgeons
- Prior Lumbar Spinal Arthrodesis Increases Risk of Prosthetic-Related Complication in Total Hip Arthroplasty
- Abnormally High Dislocation Rates of Total Hip Arthroplasty Following Spinal Deformity Surgery
- Early Outcomes of Primary Total Hip Arthroplasty after Prior Lumbar Spinal Fusion
- flexion contracture:
- not caused by the weakness of the hip extensors;
- result of contractures of the flexor muscles and the joint capsule
- to compensate for reduced hip extension in terminal stance phase & to obtain step length, there is development of increased
anterior pelvic tilt in sagittal plane;
- obesity:
- Obesity is a major risk factor for prosthetic infection after primary hip arthroplasty
- Factors associated with prolonged wound drainage after primary total hip and knee arthroplasty
- Periprosthetic joint infection: the incidence, timing, and predisposing factors.
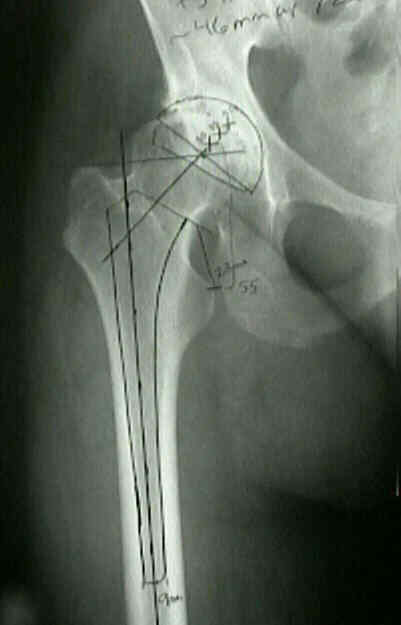
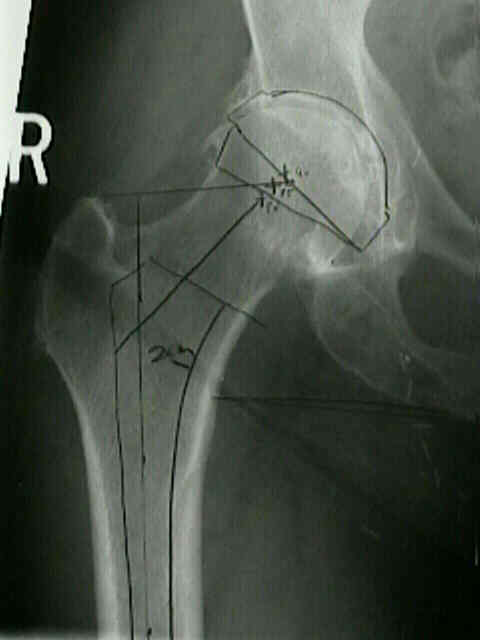
- Radiology of the Hip:
- preop acetabular evaluation: (postop eval)
- usually the acetabulum must be templated first, in order to determine the center of rotation and the center of the femoral head;



- preop femur evaluation:
- standing AP of hip, knee, & ankle;
- consider: standing AP of hip, knee, & ankle to see whether any varus or valgus deformity requires correction before THR;
- femoral offset - neck shaft angle:
- it is important to maintain the patient's original offset;
- acceptance of less femoral asset may result in abductor laxity and weakness, increased joint reactive
forces, and hip instability;
- always know ahead of time whether the implant you are using has the option of an increased offset femoral stem
in addition to knowing the modularity lengthening options of the femoral head;
- references:
- The femoral neck-shaft angle on plain radiographs: a systematic review.
- The neck shaft angle: CT reference values of 800 adult hips
- radiographic pitfalls:
- note that external rotation of the femur (as shown by a promient lesser trochanter) will give the appearance that
there is a relative coxa valga, which will give a false impression of offset;
- in femoral neck frx, the neck shaft angle cannot be judged (use opposite hip for templating);
- coxa vara, may lead to unexpected postop leg lengthening (w/ possible nerve palsy) as well as unexpected hip instability;
- consider use of a femoral stem w/ increased offset;
- references:
- The offset problem in total hip arthroplasty. Steinberg B and Harris WH. Contemp Orthop. 1992(24):556-562.
- Arthroplasty of the hip. Leg length is not important.
- Preoperative Templating and Biomechanics in Total Hip Arthroplasty
- limb length:
- draw a line at level of, & parallel to, ischial tuberosities and intersecting the lesser trochanter on each side;
- compare 2 points of intersection & measure difference to determine the amount of limb shortening;
- draw horizontal at level of proposed neck cut which may be used as a reference point during surgery;
- draw a horizontal line at the level of the greater trochanter & see where it intersects on head of femoral component;
- during surgery postion of the greater trochanter can be compared to center of the femoral prosthetic head, which gives an
indication of relative leg lengthening;
- significant leg length descrepancies can partially be adressed w/ changing prosthetic offset and partially w/ femoral neck cut;
- references:
- Preoperative Radiographic Assessment of Limb-length Discrepancy in Total Hip Arthroplasty
- The Assessment of Limb Length Discrepancy Before Total Hip Arthroplasty
- template femoral neck cut
- note that the femoral neck cut should place the center of the femoral head component at the approximate level
of the tip of the greater trochanter;
- size of component:
- place femoral templates on film & select size that matches the contour of the proximal canal and fills it most completely
- note thickness of cortex & width & shape of medullary canal;
- note amount of trochanteric back cut needed during surgery so that the stem is not placed in varus;
- w/ longer stem implants, be sure that the anterior bow to the femur will not interfere w/ insertion;
- Surgical Alternatives:
- hip arthrodesis:
- girdlestone resection arthroplasty
- references:
- Osteoarthritis of the hip treated by intertrochanteric osteotomy. A long-term follow-up.
- Medial-displacement intertrochanteric osteotomy in the treatment of osteoarthritis of the hip. A long-term follow-up study.
- Osteotomy for osteoarthritis of the hip. A survivorship analysis.
- References:
The value of preoperative planning for total hip arthroplasty.
Common Misconceptions of Normal Hip Joint Relations on Pelvic Radiographs.
Back Pain and Total Hip Arthroplasty: A Prospective Natural History Study
Predictors of Intensive Care Unit Admission After Total Joint Arthroplasty