

- See:
- Burst Frx
- Thoracic & Thoracolumbar Spine :
- Posterolateral Decompression:
- Discussion:
- frx at this level are frequently due to relative immobility of thoracic spine compared to the lumbar spine;
- upper thoracic spine (T1 to T10) is stabilized by the ribs & facet orientation, and is less suseptible to trauma;
- at T12-L1 junction, however, there is a fulcrum of increased motion & this area is more commonly affected with spine trauma;
- mechanism:
- most often results from a combination of acute hyperflexion and rotation and consequently are more unstable;
- when a person is thrown from a moving vehicle, thoracolumbar frx dislocation frequently occurs;
- lap seat belt may be assoc w/ characteristic throracolumbar flexion distraction type of injury;
- prognosis for neurologic injury:
- majority of these injuries occur at T12, L1, L2;
- neurologic injury can be purely to the cord, to the cauda equina, or a mixture of both;
- most pts w/ traumatic paraplegia sustain vertebral injury at skeletal thoracolumbar junction where conus medullaris lies, & several
lumbar roots are descending to exit thru the appropriate foramen;
- it is not a purely spinal cord injury, but involves conus medullaris and descending roots of the cauda equina;
- most thoracic injuries with significant skeletal disruption will not demonstrate neurologic return despite anatomic stabilization;
- middle of T-spine is a vascular watershed area, & vascular insult can lead to cord ischemia; (see blood supply)
- it is difficult to prognosticate about injuries at thoracolumbar junction,
where there can be mixed cord & cauda equina lesions;
- spinal cord ends & caudal equina begins at level of L1 to L2, so lesions below L1 level carry better prognosis because nerve roots
and not cord is injured;
- references:
- Neurologic injury and recovery patterns in burst fractures at the T12 or L1 motion segment.
- Neuro Exam:
- because spinal cord terminates at this level, look for bladder & bowel signs & decrease movement & sensation in lower extremities;
- Radiographs:
- recognize stable vs unstable inuries:
- three column system is helpful in evaluating spinal injuries & determining which are stable or unstable;
- at the thoracolumbar junction, more than 20 deg of kyphosis indicates an unstable frx;
- thoracolumbar injuries seldom suddenly shift position but many slowly settle into malposition over several weeks following injury;
- this is a type of unstable injury;
- thoracolumbar injuries will be stable if middle column is intact, & will be unstable if disrupted, w/ the exception of upper thoracic
spine injuries;
- above T8, injury may disrupt middle column, but frx will still be stable manner if sternum and ribs in area of injury are OK;
- chest wall tends to splint the injury site, and if chest wall is unstable the injury will be unstable;
- references:
- Sagittal index in management of thoracolumbar burst fractures.
- CT scan prediction of neurological deficit in thoracolumbar burst fractures
- The value of computed tomography in thoracolumbar fractures: An analysis of one hundred consecutive cases and a new classification.
- Thoracolumbar fracture in blunt trauma patients: guidelines for diagnosis and imaging.
- Non Operative Treatment:
- hyperextension custom orthosis;
- references:
- The nonoperative treatment of burst fractures of the thoracolumbar junction.
- An analysis of conservative (non-surgical) management of thoracolumbar fractures and fracture-dislocations with neural damage.
- The management of burst fractures of the thoracic and lumbar spine. Experience in 53 patients.
- Long-term follow-up of nonoperatively treated thoracolumbar spine fractures.
- Thoracolumbar "burst" fractures treated conservatively. A long term follow up.
- Operative Treatment:
- Posterolateral Decompression
- most indicated for unstable burst frx w/ cord impingement along w/ dural tear and nerve root entrapment
from frx of posterior elements;
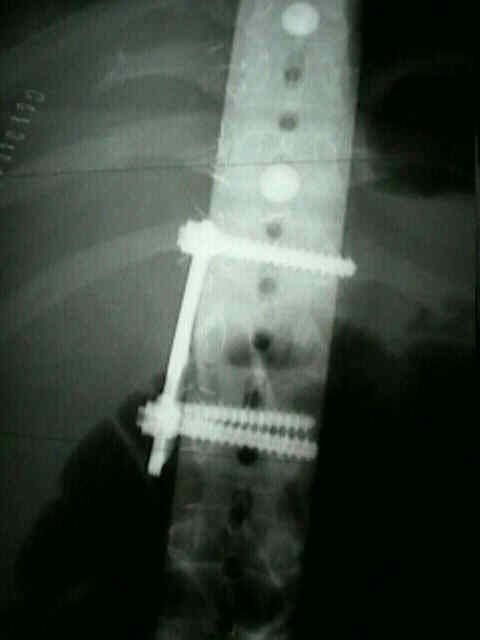
- Posterior Distraction Systems:
- Pedical Screw Implants:
- Anterior Decompression and Fusion
- most indicated for unstable burst frxs w/ cord impingement caused by bone fragments off the postero-superior vertebral body


- Complications:
- Kyphosis
Anterior fixation for burst fractures of the thoracic and lumbar spine with or without neurological involvement.
Posterior fixation of thoracic and lumbar spine fractures using DC plates and pedicle screws.
Operative neurological complications resulting from thoracic and lumbar spine internal fixation.
Anterolateral compression fracture of the thoracolumbar spine. A seat belt injury.
A new type of fracture-dislocation of the thoracolumbar spine.
Transpedicular fixation of thoracolumbar vertebral fractures.
Complications following Harrington instrumentation for fractures of the thoracolumbar spine.
Surgical management of thoracolumbar spine fractures with incomplete neurologic deficits.
Neurologic injury and recovery patterns in burst fractures at the T12 or L1 motion segment.
Early rod-sleeve stabilization of the injured thoracic and lumbar spine.
Complications of anterior approaches to the thoracolumbar spine. Emphasis on Kaneda instrumentation.
Evaluation of surgical treatment for burst fractures.
Comparison of operative versus nonoperative treatment of lumbar burst fractures.