


- Discussion:
- fall from a height, landing on one's feet, is typical of this fracture;
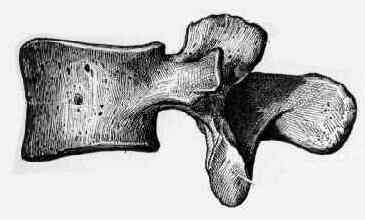
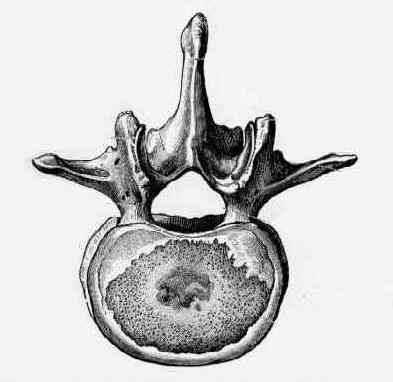
- burst frx involve only compressive failure of vertebral body both anteriorly & posteriorly, w/ failure of both anterior & middle columns;
- axial loading applied to intravertebral disc results in increased nuclear pressure and hoop stresses in the annulus;
- this results in a high shear stress on the vertebral end plate at inner border of the annulus, away from center of disc;
- a large central posterior-superior fragment occurs as a result of these forces;
- Burst Frx Location:
- Cervical Burst Frx
- Lumbar Burst Frx:
- Thoracic Burst Frx:
- Thoracolumbar Burst Frx:
- Classification: (stable or unstable)
- stable frx:
- neurologically intact;
- posterior arch remains intact: pedicle widening implies post arch disruption w/ instability;
- less than 50% anterior body height collapse:
- compression fractures:
- unstable frx:
- neurologic deficit;
- loss of 50% of vertebral body height;
- fracture dislocation:
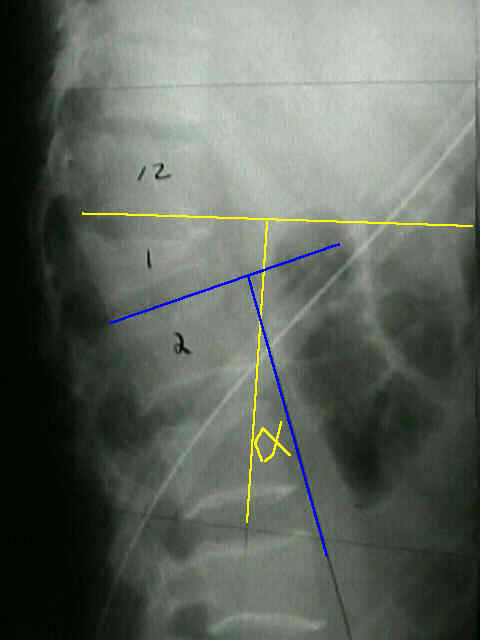
- thoracolumbar burst frx:
- angulation of the thoracolumbar junction > 20 deg
- canal comprimise > 30 percent
- Examination:
- inaddition to the orthopaedic examination, the patient should be evaluated for an ileus;
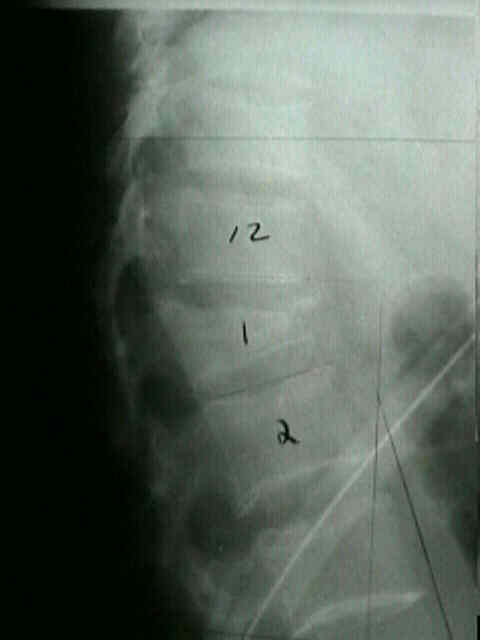
- Radiographs and Classification
- in thoracolumbar burst frx, look for comminution of the postero-superior corner of vertebral body;
- good quality AP radiographs are necessary to visualize the posterior elements;
- ensure that appropriate radiographs have been taken to rule out other concomitant injuries (such as pelvic frx);


- CT scan:
- allows assessment of canal comprimise and better visualization of posterior element injury;
- Initial Managment:
- see: management of spine injured patient
- w/ neurologic injury steroids may be indicated;
- its essential that the patient be log roled off the trauma board as soon as possible (inorder to avoid devastating pressure ulceration);
- ileus (common associated condition);
- in some cases an NG tube is required for severe ileus;
- if bowel sounds and flatus are not present then patient should be made NPO, and should receive IV fluids;
- Non Operative Treatment:
- most stable burst fractures and most lumbar burst fractures can be treated non operatively;
- w/ non operative treatment, significant remodeling and reabsorption (about 50%) of retro-pulsed fragments can be expected to occur;
- relative contra-indications:
- unstable burst frx;
- morbid obesity
- presence of associatted conditions which would preclude brace wear;
- total contact orthosis (w/ or w/o hyperextension) is worn for 4-6 months;
- leg extension must be added for fractures below L3;
- typically patients are allowed out of bed 3 to 14 days after injury, unless there are other concomitant injuries such as pelvic frx;
- whereas initial radiographs are taken supine, w/ long term follow up, radiographs need to be taken standing to evaluate for kyphosis;
- reference:
- Conservative treatment of fractures of the thoracic and lumbar spine.
- Nonoperative treatment of thoracic and lumbar spine fractures: a prospective randomized study of different treatment options.
- Operative Treatment:
- Posterolateral Decompression
- most indicated for unstable burst frx w/ cord impingement along w/ dural tear and nerve root entrapment from frx of posterior elements;
- Posterior Distraction Systems:
- Pedical Screw Implants:
- Anterior Decompression and Fusion
- most indicated for unstable burst frxs w/ cord impingement caused by bone fragments off the postero-superior vertebral body


- Complications:
- Kyphosis
Magnetic resonance imaging after pedicular screw fixation of the spine.
Evaluation of surgical treatment for burst fractures.
Dural laceration occurring with burst fractures and associated laminar fractures.
Evaluation of surgical treatment for burst fractures.
Mechanical comparison of anterior spinal instrumentation in a burst fracture model.
The "fixateur interne" as a versatile implant for spine surgery.