- Discussion:
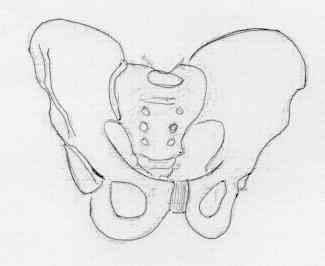
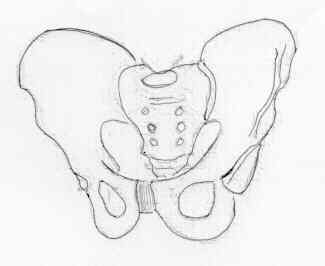
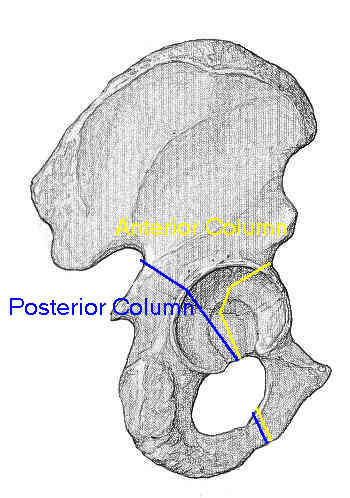
- anterior column extends from symphysis pubis & obturator foramen thru
acetabulum to ASIS and up through iliac crest;
- anterior column is less frequently fractured than posterior column due to frequency
of posteriorly directed forces;
- frxs of the anterior column may comprimise any portion of the column;
- fracture line may extends from the middle of the pubic ramus to any point above
anterior segment of the iliac crest;
- most commonly, anterior column fracture exits below anterior inferior iliac spine;
- distal anterior column fractures:
- from exam of CT scan, look for frxs of superior pubic ramus which may
enter inferior portion of acetabulum, violating joint;
- frx of anterior column frequently occur in middle or articular segment;
- in this region bone is relatively thin and overlies the joint;
- there is often comminution into quadrilateral plate surface;
- area is less accessible becuase of overlying iliopsoas muscle & obturator internus muscle;
- associated injuries: anterior hip dislocation;
- Radiographs:
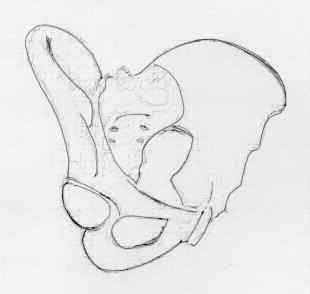
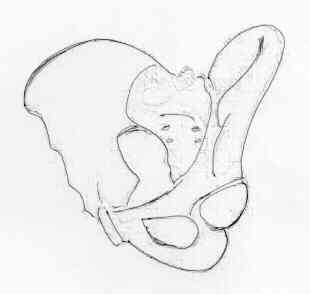
- Internal (Obturator) Oblique View:
- visualizes iliopubic / iliopectineal line of pelvis & posterior acetabular rim;
- disruption of the iliopectineal line indicates anterior column frx;
- technique:
- patient is supine w/ involved side of pelvis rotated anteriorly 45 deg;
- central beam directed vertically toward the affected hip;
- Indications for Operative and Non Operative Treatment:
- CT scan can give an indication of the amount of involvement of the wt bearing dome;
- in the study by Vrahas MS, et al (1999), a cadaveric biomechanical study was performed to determine the relative stability of
anterior column, posterior column, and transverse fractures;
- they noted that anterior column fractures with an anterior roof-arc angle (obturator oblique radiograph) of 25 degrees or less
were unstable and required ORIF;
- fractures which fall outside of this zone can potentially be treated non operatively;
- ref: The effects of simulated transverse, anterior column, and posterior column fractures of acetabulum on stability of hip joint.
- Non Operative Treatment:
- fractures must fall outside of the danger zone (roof-arc angle on obturator oblique radiograph of 25 degrees) and hip reduction
must be congruent;
- in some cases, traction is necessary to maintain the reduction;
- if once the patient is mobilized, new radiographs can be taken to ensure that the frx postion has not shifted;

- Surgical Treatment:
- surgical approach: ilioinguinal
- frx of anterior column are exposed using ilioinguinal approach w/ supine positioning;
- reduction and initial fixation:
- initial fixation of anterior column may require interfragmentary screws & plates to stabilize frx
of iliac wing, depending on fracture type;
- during reduction, reestablishment of pelvic brim allows reconstruction of entire anterior column (iliac fossa is more concave
than is often appreciated);
- initial reduction reduction may be obtained w/ lateral traction applied by a half pin inserted in the femoral neck;
- percutaneous fixation: (Internal (Obturator) Oblique View:)
- Modified Iliac Oblique-Outlet View: A Novel Radiographic Technique for Antegrade Anterior Column Screw Placement.
- Percutaneous Fixation of Anterior and Posterior Column Acetabular Fractures
- Axial view of acetabular anterior column: a new X-ray projection of percutaneous screw placement
- implants: synthes implants
- early application of precurved plates simplifies the reduction;
- plate is slide underneath musculature of iliopsoas and femoral vessels;
- plate attached to body of pubis w/ a screw & then plate is rotated along superior pubic ramus until it
sits congruently on
 iliopectineal line and pelvic brim;
iliopectineal line and pelvic brim; - plate extends posteriorly along pelvic brim from posterior part of iliac fossa and anteriorly to
pubic symphysis;
- screw purchase is best obtained far medially on superior pubic ramus and posteriorly, in iliac wing;
- because frx of ischiopubic ramus are difficult to reach & do not appear to significantly influence end
results, no attempt is made to stabilize this component of the fracture;
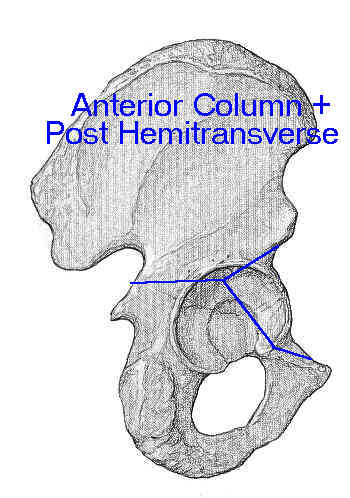
- Biomechanical analysis of fixation systems for anterior column and posterior hemi-transverse acetabular fractures.
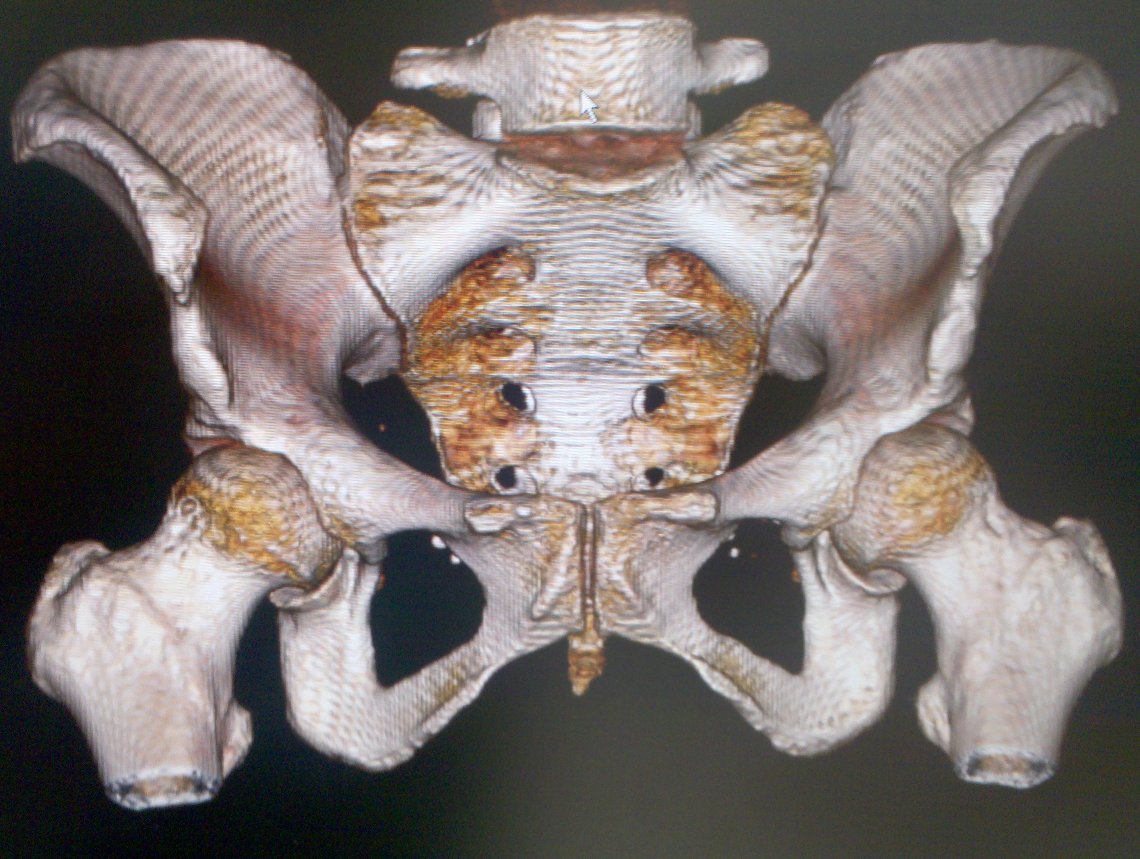
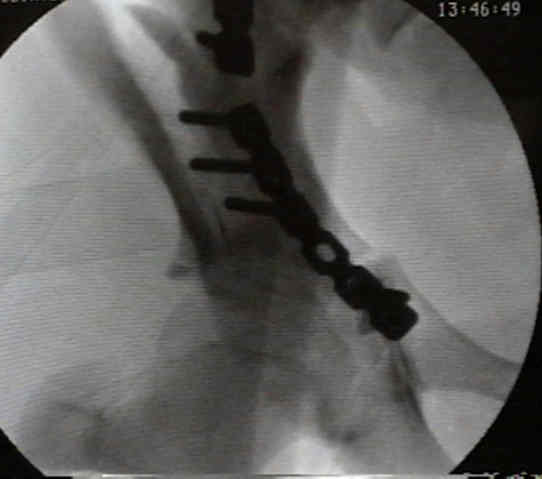
- Case Example:
25 year old male involved in MVA, sustaining an iliac wing fracture and a low transverse acetabular frx;



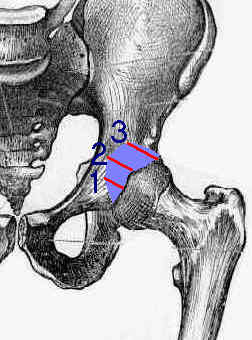
- Danger Zone: (from Benedetti et al. 1996)
- diagram shows danger zone at 1, 2, and 3 cm above the inferior acetabulum rim;
- in general the danger zone extends about 2.5 cm medially from the acetabular rim;
- Screw Placement into the Anterior Column:
- applicable for T-type frx, transverse frx, and both column frx;
- 1 cm above the inferior edge of the acetabulum:
- at 0.5 mm lateral to the pelvic brim, screw are inserted at 25 deg of medial angulation
(screw length 20 mm);
- at 1.0 cm lateral to the pelvic brim, screw are inserted at 35 deg of medial angulation (screw length
20-25 mm);
- at 1.5 cm lateral to the pelvic brim, screw are inserted at 45 deg of medial angulation (screw length 25 mm);
- 2 cm above the inferior edge of the acetabulum:
- at 0.5 mm lateral to the pelvic brim, screw are inserted at 30 deg of medial angulation (screw length 20 mm);
- at 1.0 cm lateral to the pelvic brim, screw are inserted at 40 deg of medial angulation (screw length 20-25 mm);
- at 1.5 cm lateral to the pelvic brim, screw are inserted at 50 deg of medial angulation (screw length 25 mm);
- 3 cm above the inferior edge of the acetabulum (level of ASIS):
- at 0.5 mm lateral to the pelvic brim, screw are inserted at 20 deg of medial angulation (screw length of 45 mm);
- at 1.0 cm lateral to the pelvic brim, screw are inserted at 30 deg of medial angulation (screw length of 45-50 mm);
- at 1.5 cm lateral to the pelvic brim, screw are inserted at 40 deg of medial angulation (screw length of 50 mm)
- Percutaneous Screw Placement
The “safe zone” for infrapectineal plate-screw fixation of quadrilateral plate fractures: An anatomical study and retrospective clinical evaluation
Anterior column fractures of the acetabulum.
Anatomic Considerations of Plate-Screw Fixation of the Anterior Column of the Acetabulum.
Percutaneous Fixation of the Columns of the Acetabulum. A New Technique.
Percutaneous Screw Fixation of Acetabular Fractures: Applicability of Hip Arthroscopy
The Pararectus Approach A New Concept
- PreOp Planning: