

- See:
- Classification and Column Theory
- Posterior Wall Fractures
- AO Foundation Posterior Column Frx
- Discussion:
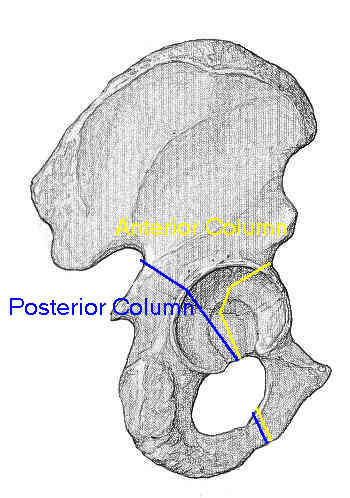
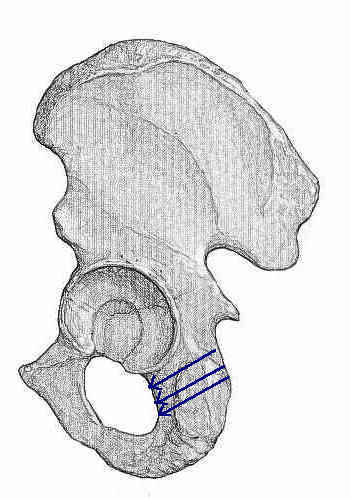
- posterior column extends from obturator foramen thru posterior aspect of the wt bearing dome
of acetabulum & then obliquely through greater sciatic notch;
- frx of posterior rim & posterior column arise from MVA, most likely as result of dashboard impact;
- associated injuries:
- posterior dislocation of the femur
- AP compression frx
- Radiographs:
- posterior column fractures involve not only posterior articular surfaces, but also the ilioischial line;
- AP view:
- medial displacement of the femoral head and sciatic buttress;
- ilioishial line is disrupted;
- external (iliac) oblique view:
- visualizes ilioischial (posterior) column & anterior acetabular rim;
- often reveals the internal and superior boundaries of the displaced fragment;
- radiographic technique: pt is supine w/ uninvolved side rotated anteriorly 45 deg and central beam directed
vertically toward the affected hip
- assesment of stability:
- in the study by Vrahas, et al (1999), a cadaveric biomechanical study was performed to determine the relative stability of
anterior column, posterior column, and transverse fractures;
- they noted that posterior column frx w/ posterior roof-arc angle (iliac oblique radiograph) of 70 degrees or less were
unstable and required ORIF;
- references:
- The effects of simulated transverse, anterior column, and posterior column fractures of the acetabulum on the stability of the hip joint.
- PreOp Planning: 
- work up of acetabular frx:
- w/ posterior injury, the sciatic nerve may be injured in 40% of patients;
- Surigical Approach:
- Kocher-Langenback incision is used w/ pt in prone position;
- dislocation of femoral head:
- Surgical Hip Dislocation for Exposure of the Posterior Column
- Reduction:
- sciatic notch is useful landmark to help reconstruct posteror column;
- posterior column is strong & triangular, w/ extremely thick bone at greater trochanter sciatic notch;
- medial surface forms posterior aspect of quadrilateral plate;
- reduction may achieved w/ direct visualization of quadrilateral surface thru distraction of femur if needed, & thru palpation
of quadrilateral surface through greater sciatic notch (through posterior approach);
- insertion of Schanz screw:
- w/posterior approach, reduction is by inserting a Schanz screw into the ischium just inferior to the subcotyloid gutter;
- T chuck is applied over Schanz screw, which is then used to rotate a displaced posterior column frx into a reduced position;
- the surgeon's other hand can guide the reduction by palpating the quadrilateral surface;
- additionally a Schanz screw may be placed into the greater trochanter for additional traction;
- frx lines may be distracted using lamina spreader or AO femoral distractor;
- frx lines may be compressed using Farabeuf clamps;
- blood clot & granulation tissue are removed, as are any free fragments that might impede reduction;
- identify & reduce marginally impacted frx of posterior wall;
- Reconstruction:
- posterior column is reconstructed using lag screws or pelvic recon plates;
- initial fixation is w/ lag screw, placed from posterior to anterior & followed by a curved plate on the retroacetabular surface;
- small reconstruction plate applied from the ischial tuberosity to the lateral ilium along the retroacetabular surfaces.
- Screw Placement in the Ischial Tuberosity:
- anatomical hazards:
- internal pudendal bundle usually lies 1.5 cm from the medial posterior margin of
ischial tuberosity;
- internal pudendal bundle passes out of greater sciatic foramen, passes around
sacrospinous ligament, over the internal obturator muscle (just medial to the
tuberosity) and then into lesser foramen;
- excessively medially angulated screws may injure the internal pudendal;
- at 2 cm below the inferior acetabular margin, hamstring origin is encountered (and therefore
dissection below this point is avoided);
- technique of insertion:
- maximal purchase is achieved w/ entry into the tuberosity 5 or 10 mm medial to the lateral margin
of the tuberosity and are directed inferiorly;
- at the level of the inferior acetabular margin, direct the screw 35-40 deg caudally;
- at 1 cm below the inferior acetabular margin, direct screws 45-50 deg caudally;
- at 2 cm below the inferior acetabular margin, direct screws 50-55 deg caudally
Modified technique of percutaneous posterior columnar screw insertion and neutralization plate for complex acetabular fractures
www.ncbi.nlm.nih.gov/pmc/articles/PMC6485765/
Transgluteal Posterior Column Screw Stabilization for Fractures of the Acetabulum: A Technical Trick
Custom-made Locked Plating for Acetabular Fracture: A Pilot Study in 24 Consecutive Cases
Percutaneous Fixation of Anterior and Posterior Column Acetabular Fractures