

Discussion
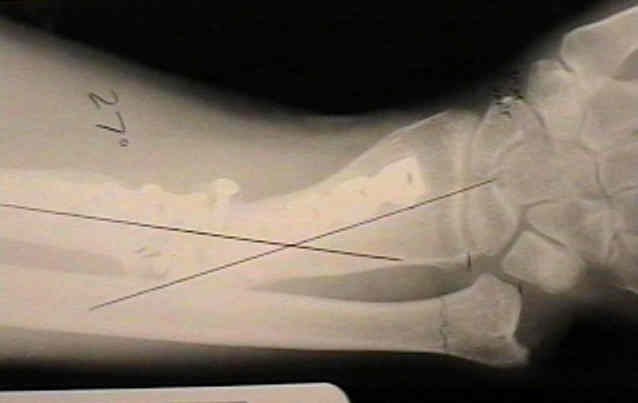
- frx of radial shaft (between middle and distal 1/3's) & dislocation of distal radioulnar joint;
- usually the dislocation is dorsal, but in some cases can be palmar;
- frx is almost always located just above proximal border of pronator quadratus;
- usually there is anterior angulation w/ transverse or short oblique config;
- RU joint injury:
- may be purely ligamentous (tearing the TFCC)
- ligament complex may remain intact and the ulnar styloid may be avulsed
- in children there may be separation of the distal ulnar epiphysis
- mechanism: usually direct blows and falls;
- displacing forces:
- wt of hand tends to cause subluxation of distal RU joint & dorsal angulation of the frx radius;
- insertion of pronator quadratus on palmar surface of distal fragment rotates it toward ulna & pulls it in prox & palmar direction;
- brachioradialis causes shortening & rotation of distal RU joint
Treatment in Children
- Variant of Galeazzi fracture-dislocation in children.
- Galeazzi-equivalent injuries of the wrist in children.
Surgical Treatment in Adults
- see plating techniques:
- adults tend to have poor results with closed reduction;
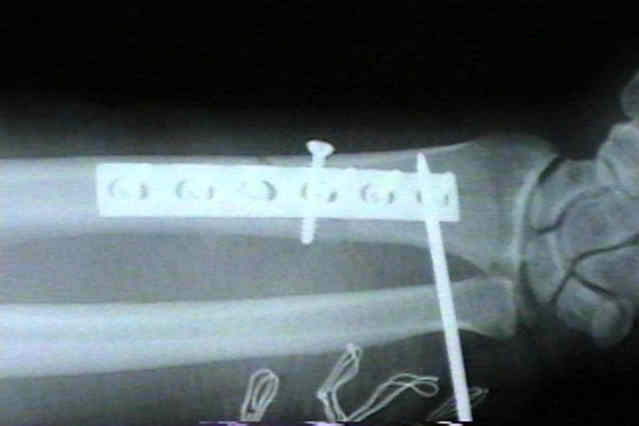
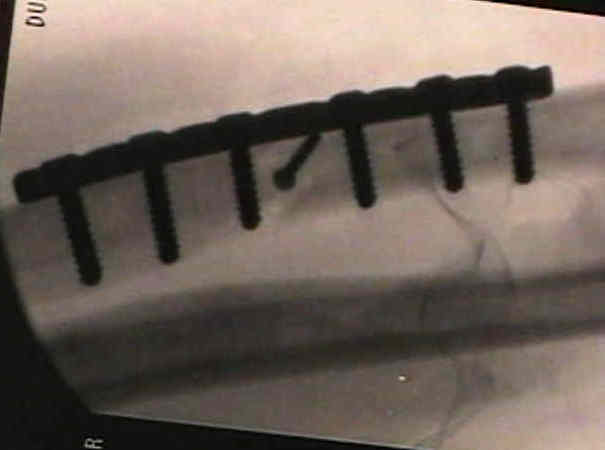
- most adults require compression plates & screws (see below);
- w/ pure transverse frx, 4 hole 4.5 mm plate or 6 hole 3.5 mm plate is acceptable, but if there is comminution a larger plate is necessary;
- no screw should be w/ in 1 cm of frx;
- references:
Surgical Approach
- Anterior Approach of Henry;
- 5-6 inch longitudinal incision is made, centered over frx in plane between FCR which is retracted ulnarly and BR;
- radial artery is identified & retracted to ulnar side;
- BR & superficial radial nerve are retracted radially;
- frx is located just above proximal border of pronator quadratus;
- insertion of pronator quadratus is freed from radius & reflected ulnarward;
RU Joint
- following fixation of the radius, need to reevaluate distal RU joint;
- it is often difficult to evaluate stability of the RU joint w/o opening and directly visualizing the joint;
- the closer the radius fracture is to the DRUJ, the more likely it is to be unstable;
- even if the supinated joint appears to reduce under flouro, the surgeon's fingers may palpate gross dorsal subluxation;
- in the report by Rettig ME and Raskin KB, the authors categorized these fracture into type I (fractures within 7.5 cm of midarticular surface of the distal radius) and type II fractures (greater than 7.5 cm from joint surface);
- 22 fractures were type I, and 12 of these cases were associated with intraoperative DRUJ instability;
- 18 type II fractures and were type II, and only one of these frx had intraoperative DRUJ instability after ORIF;
- surgical fixation:
- have the surgical assistant partially supinate the patient's arm
- the surgeon's non dominant hand keeps the joint reduced and helps to "triangulate the k wire" which is driven in with the surgeon's dominant hand;
- if RU joint is unstable, then K wire fixation is required (K wires are inserted from the ulnar into the radius);
- references:
- Galeazzi fractures: Is DRUJ instability predicted by current guidelines?
- Distal radioulnar joint function after Galeazzi fracture-dislocations treated by open reduction and internal plate fixation.
- Distal Radioulnar Joint Instability (Galeazzi Type Injury) After Internal Fixation in Relation to the Radius Fracture Pattern.
Post Op
- classic recommendations include, ORIF followed by immobilization in long arm cast with forearm in full supination for 6-8 weeks;
- references:
Complications
Entrapment of extensor tendons
- ECU is usually affected but may occur in EDM
- ulnar styloid may sustain avulsion frx & displace into distal RU joint with the extensor carpi ulnaris tendon.
- exam reveals a vacant ECU sulcus (empty sulcus sign);
- distal radio-ulnar joint is irreducible even after ORIF of radial frx;
- ECU will be found either in RU joint or displaced in an ulnar direction around ulnar head;
Treatment
- to avoid chronic instability, the distal radio-ulnar joint is reduced & ECU tendon sheath is repaired;
- surgical repair includes open reduction of distal RU joint, suture repair of ECU fibro-osseous canal, & ORIF of ulnar styloid frx;
RU joint subluxation
- Distal radioulnar joint function after Galeazzi fracture-dislocations treated by open reduction and internal plate fixation.
- Distal Radioulnar Joint Instability (Galeazzi Type Injury) After Internal Fixation in Relation to the Radius Fracture Pattern.
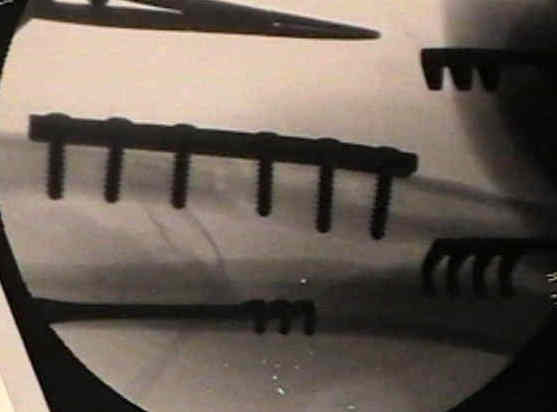
Case example

- 30 yo WM who initially underwent ORIF of a Galeazzi frx w/o pin fixation of the RU joint;
- several weeks lateral RU joint diastasis occur which required closed pinning as a second procedure;



References
- Results of compression-plating of closed Galeazzi fractures.
- Galeazzi injury with an associated fracture of the radial head.
- Unstable fracture-dislocations of the forearm (Monteggia and Galeazzi)
- Galeazzi fracture-dislocations.
- Management of the Galeazzi fracture.
- Complex volar distal radioulnar joint dislocation occurring in a Galeazzi fracture.
- Internal fixation in 50 cases of Galeazzi fracture.
- The Interosseous Membrane of the Forearm: Structure and Its Role in Galeazzi Fractures.
- Galeazzi fractures.
- Variant of Galeazzi fracture-dislocation in children.
- Galeazzi-equivalent injuries of the wrist in children.