


- See:
- Rheumatoid Hand
- MP Ulnar Drift
- Deformites of MP Joints;
- approximately 40% of pts w/ RA will have intrinsic contracture;
- in some cases the intrinsic contracture will result from MP joint dislocation, and in other cases, the intrinsic contracture will be idiopathic (and may result in MP dislocation);
- as the intrinsic tightness progresses (as determined by Bunnel test), either MP subluxation will occur or the constant pull of the intrinsics will cause a swan neck deformity beginning at the PIP joint;
- when MP subluxation occurs, tension will be taken off the intrinsics, which then allows full PIP flexion when the MP joint is extended;
- w/ rheumatoid involvement of MP joint, there will be weakening & elongation of MP capsule & collateral ligaments;
- as resistance to displacing forces is lost, extensor tendons are displaced in an ulnar and palmar directions;
- flexor tendons enter fibrous sheath at angle, exerting ulnar & palmar pull that is resisted in the normal hand;
- as a result base of proximal phalanx moves ulnarly and palmarly;
- 4th & 5th metacarpals are esp at risk for ulnar drift because of their increased mobility;
- loosening of ligaments at carpometacarpal joints & dysfunction of ECU tendon also play a role; (ulnar head syndrome);
- increased ulnar drift, subluxation of extensor tendons, and palmar subluxation of joints are the end result;
- classification:
- index MP joint deformity:
- pronation deformity of index finger is common in the RA hand;
- in normal hand, pinch between thumb & index finger requires slight supination of index finger so that palmar surfaces can meet;
- in pronation deformity, less useful lateral surfaces are opposed;
- during pinch, pronation deformity is seen in all three joints, but it is more pronounced in the MP joint;
- arthroplasty of this joint should include recontruction of capsulo-ligamentous and musculotendinous systems;
- diff dx:
- MP joint dislocation: failure of digit extension from chronic dislocation of MCP:
- pt can maintain extension achieved passively
- bouvier's test
- PIN syndrome:
- tenodesis effect present - not present with rupture
- trigger finger (no passive movement possible);
- extensor tendon rupture
- examination of the extensor tendons can be difficult w/ concomitant MCP dislocations and PIP joint pathology;
- attempt to palpate the tendons over the metacarpal head as the patient makes a major effort to extend the fingers;
- extensor tendon pathology should be suspected if there there is concomitant caput ulna syndrome;
- MP Joint Treatment Options:
- synovectomy
- extensor mechanism relocation
- intrinsic tendon release
- arthroplasty
- PreOp Planning:
- goals of treatment:
- pain relief, improved f(x), preventing further damage, cosmesis;
- concomitant wrist disease:
- healthy axiom for surgery in RA is to start proximally & work distally alternating fusion with motion sparing procedures;
- hence consider adressing wrist disease before MP disease;
- correctable radial deviation deformity:
- if deformity is passively correctable, consider tendon transfer ECRL, to the ECU tendon;
- generally radial deviation deformity of the wrist should be corrected prior to MTP arthroplasty;
- concomitant extensor tendon rupture:
- the traditional teaching is that synovectomy and extensor tendon repair should procede MCP arthroplasty by 6 to 8 weeks;
- some surgeons, however, will elect to perform both the MCP arthroplasty and the extensor tendon reconstruction at the same time, noting that it is difficult to properly tension the tendon reconstruction when the MCP joints are dislocated;
- concomitant PIP deformity:
- if both MP & PIP joints are involved, the MP joint is usually treated first;
- w/ swan neck deformity, MP & PIP joints are reconsturcted at same stage;
- w/ boutonniere deformity, PIP is reconstructed first;
- tendon imbalances and joint malalignment must be corrected;
- implant arthroplasty for both the MP and PIP joints of the same digit is usually not recommended;
- severe deformity of both MCP & IP joints of thumb w/ intact CMC joint is indication for arthrodesis of both MCP & IP joints;
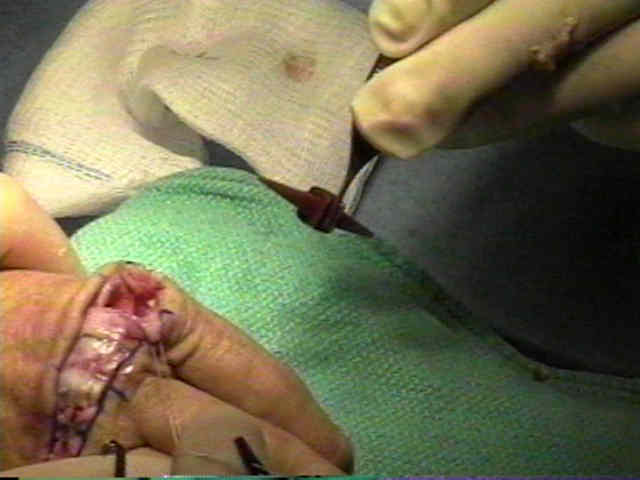
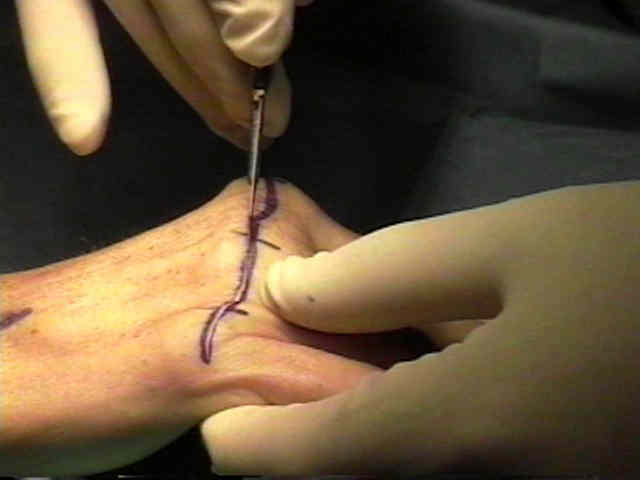
- MP Joint Arthroplasty:
- for progressive MPJ ulnar drift
A simplified technique to correct hyperextension deformity of the metacarpophalangeal joint of the thumb.
Flexible (silicone) implant arthroplasty of the metacarpophalangeal joint of the thumb.
Fusion of the first metacarpotrapezial joint for degenerative arthritis.
Post-traumatic instability of the metacarpophalangeal joint of the thumb.
Motion after metacarpophalangeal joint reconstruction in rheumatoid disease.