

- Discussion:
- impingement syndrome describes pain in subacromial space when the humerus is elevated or internally rotated;
- during humeral flexion, the supraspinatus tendon and bursa become entrapped between the anteroinferior corner of the acromion
(and CA ligament) and the greater tuberosity;
- this syndrome is thought to precipitate attritional changes in the rotator cuff, leading to RTC tear;
- once the supraspinatus (and infraspinatus) tendon is disrupted there will often be further impingement and irritation which
can lead to biceps tendonitis and subsequent rupture;
- differential diagnosis
- staging of impingement syndromes
- outlet impingement:
- rotator cuff and subacromial bursa can be impinged between the greater tuberosity and the:
- anterior 1/3 of acromion:
- greater tuberosity impinges anteriorly w/ forward flexion and laterally along undersurface of the acromion with modest
abduction and neutral rotation;
- similar phenomenon can occur after displaced AC separations;
- coracoacromial ligament:
- forced internal rotation in forward flexed position will drive greater tuberosity against the CA ligament;
- AC joint:
- AC arthritis or AC joint osteophytes can result in impingement and mechanical irritation to the rotator cuff tendons;
- misc causes: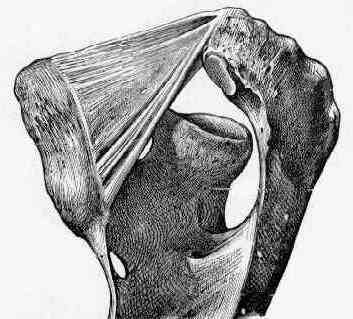
- greater tuburosity fractures can cause impingement on the rotator cuff if the fragment rotates superiorly;
- humeral neck fractures that heal in a varus position will cause the greater tuberosity to tilt more superiorly;
- coracoid impingement:
- pain is lower and more anterior than with superior impingement;
- look for decreased horizontal adduction with pain similar AC disease, but the pain is at tip of the
coracoid and not AC joint;
- subscapularis tendon and biceps degeneration and partial tearing are associated with this type of impingement;
- non-outlet impingment:
- loss of normal humeral head depression by the rotator cuff tear or weakness from a C5-6 lesion or suprascapular nerve palsy, or biceps tendon rupture;
- may occur due to thickening or hypertrophy of the subacromial bursa and rotator cuff tendons;
- may occur in the throwing athlete due to posterior impingement;
- in these cases, patients may demonstrate excessive external rotation and/or recurrent anterior instability;
- references:
- Posterior Capsular Contracture of the Shoulder
- Arthroscopic capsular release for painful throwing shoulder with posterior capsular tightness.
- Quantifying Acromiohumeral Distance in Overhead Athletes With Glenohumeral Internal Rotation Loss and the Influence of a Stretching Program
- Clinical Findings: (see shoulder exam)
- staging of impingement syndromes
- pain will often become worse at night, as the subacromial bursa becomes hyperemic after a day of activity;
- impingement test is performed by 1st eliciting positive impingement sign;
- impingement sign: pain which occurs after forward flexing arm to 90 deg, and forcefully internally rotating the shoulder;
- 10-15 ml of 1% xylocaine are the injected into the subacromial space, and the impingement sign is again sought;
- subacromial space should not be injected with steroids twice, because of the risk of tendon rupture;
- carefully test for shoulder contractures:
- patients w/ contracture of posterior capsule (and loss of IR) will be most likely to demonstrate signs of impingement (despite normal acromial anatomy);
- ref: Quantification of Posterior Capsule Tightness and Motion Loss in Patients with Shoulder Impingement
- Radiographic Classification:
- scapular outlet view
- 30 deg caudal tilt AP view
- this is perhaps the most important radiographic study since it shows the anterior proliferation of the anterior acromion relative to
clavicle (which cannot be determined from the outlet radiograph);
- Non-Operative Treatment:
- as noted by Morrison, et al (1997), 2/3 of patients can expect to have significant relief of symptoms with non operative treatment;
- only half of patients who are over 60 years of age will have satisfactory result with non operative treatment;
- 91% of patients w/ a type I acromion will have satisfactory result;
- patients should specifically work on increasing specific deficits in their ROM such as loss of internal rotation (as compared to the normal side);
- specific techniques:
- IR is improved by having the patient reach the good hand behind his neck and and simultaneously place his painful side in
maximal IR up the back;
- a towel or a rope is used to connect the two hands, and the good hand raises up to celing, forcing the other into maximal internal rotation;
- flexion is improved on by use of overhead pulleys and use of a meter stick;
- Non-operative treatment of subacromial impingement syndrome.
- Operative Treatment:
- cases that do not respond to above conservative measures after 6 months of treatment are candidates for surgery;
- choices include open acromioplasty or arthroscopic acromioplasty;
- note that Rockwood and Lyons expressed concern about arthroscopic decompression because it disrupts the lower half of the deltoid origin to the deltoid;
- while this concern has not been borne out by clinical studies, it may be an important consideration for type III acromions, since
an adequate decompression would require an extension amount of deltoid detachment both inferiorly and anteiorly;
- ref: Shoulder impingement syndrome: diagnosis, radiographic evaluation, and treatment with a modified Neer acromioplasty.
- preoperative considerations:
- be clear with the patient about the expected results of surgery;
- if the patient demonstrated excessive pain from the subacromial steroid injection (at the time of injection), then it is likely that
the patient will demonstrate excessive postoperative pain;
- likewise, if the results of the steroid injection did not provide significant relief, then a decompression may not satisfy the patient's expectations;
- cautions:
- in the case of massive rotator cuff tear, an acromioplasty (w/ CA ligament release) may precipitate additional superior migration;
- throwing athelets w/ impingment often do not benefit from acromionplasty
Failed acromioplasty for impingement syndrome.
Anterior acromioplasty for subacromial impingement in patients younger than 40 years of age.
Impingement syndrome in the absence of rotator cuff tear (stages 1 and 2).
Subacromial impingement decompressed with anterior acromioplasty.
The Weight-Bearing Shoulder. The Impingement Syndrome in Paraplegics.