

- Discussion:
- indicated for displaced surgical neck, 3 part, and 4 part fracture;
- deforming forces:
- pectoralis major pulls the shaft medially, anteriorly and internally rotates;
- supraspinatus abducts the head fragment in two part fractures;
- w/ greater tuberosity is fracture, it will be pulled superiorly and posteriorly by the supraspinatus and infraspinatus;
- lesser tuberosity will be found attached to subscapularis and the rotator cuff to the greater tuberosity;
- often two are combined as a single fragment, with the long head of biceps tendon running thru it;
- Anterior Approach to Shoulder:
- incision is made along medial border of deltoid extending laterally to humeral shaft;
- cephalic vein protected;
- superior part of pectoralis may have to be divided;
- deltoid detachment:
- when greater access to proximal humerus is required, more extensive removal of deltoid is required;
- w/ need for additional exposure, deltoid muscle should be removed from clavicle by raising an osteoperiosteal flap laterally to the acromion;
- references:
- The sub-deltoid approach to the metaphyseal region of the humerus.
- The extended deltoid-splitting approach to the proximal humerus.
- The extended anterolateral acromial approach allows minimally invasive access to the proximal humerus.
- Lessons learned from a case of proximal humeral locked plating gone awry.
- Assessment of axillary nerve function and functional outcome after fixation of complex proximal humeral fractures using the extended deltoid-splitting approach.
- The Plate-Joystick Technique to Reduce Proximal Humeral Fractures and Nonunions With a Varus Deformity Through the Extended Deltoid-Splitting Approach
- Locked plating for proximal humeral fractures: differences between the deltopectoral and deltoid-splitting approaches
- Locking Plate Fixation Techniques: (Synthes locking plate 3.5 LCP: vs LCP periarticular plate)
- surgical considerations:
- flouro setup:
- rotate the table 180 deg so that the foot portion of the table is under the patient's head;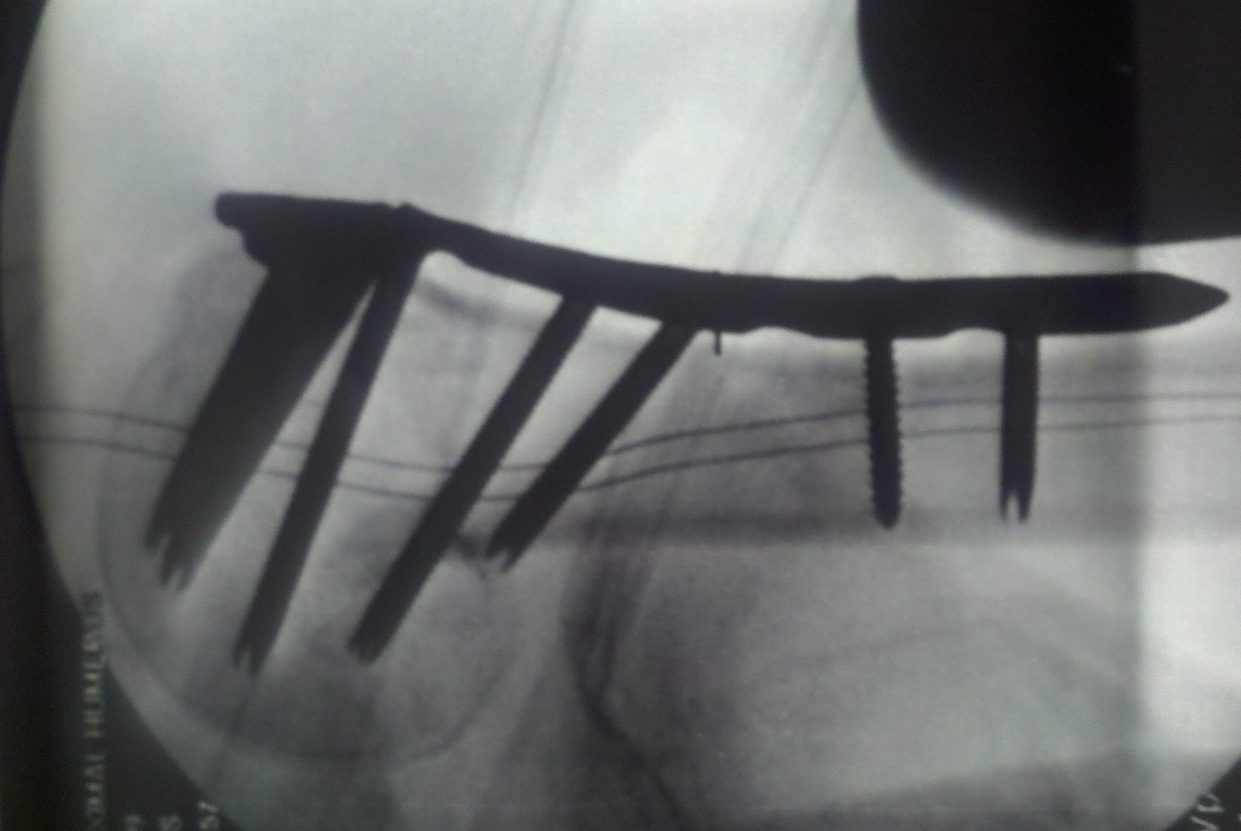
- flouroscope is placed proximal to the head of the table, parallel with the table;
- intraoperative fracture reduction
- references:
- The biomechanics of locked plating for repairing proximal humerus fractures with or without medial cortical support.
- Factors that influence Reduction Loss in Proximal Humerus Fracture Surgery.
- Reducing Postoperative Fracture Displacement After Locked Plating of Proximal Humerus Fractures: Current Concepts.
- How to enhance the stability of locking plate fixation of proximal humerus fractures? An overview of current biomechanical and clinical data.
- Medial calcar support and radiographic outcomes of plate fixation for proximal humeral fractures.
- assessment of rotator cuff:
- ref: Prevalence of Rotator Cuff Tears in Operative Proximal Humerus Fractures
- plate position:
- plate is positioned at least 8-15 mm distal to the upper end of the greater tuberosity (different plate
designs will have specific plate distances);
- subacromial impingement may occur if the plate is positioned too far cranially
- plate is applied immediately lateral to the bicipital groove;
- remember that there is typically 30 humeral retroversion, so that the plate needs to be directed posteriorly into the body of the humeral head;
- in some cases, the plate is judiciously applied upto the tuberosity edge (high enough to capture the tuberosity fragment;
- ensure that plate impingement is not present;
- insert most proximal locking screw first to ensure that plate is distal enough;
- tuberosity reduction may be more important than impingement (because the plate can later be removed);
- plate fit is perhaps the least important;
- references:
- Lessons learned from a case of proximal humeral locked plating gone awry.
- Pitfalls and complications with locking plate for proximal humerus fracture
- screw insertion and optimal screw position:
- optimal screw purchase with respect to bone fixation can be achieved by including screws located in the 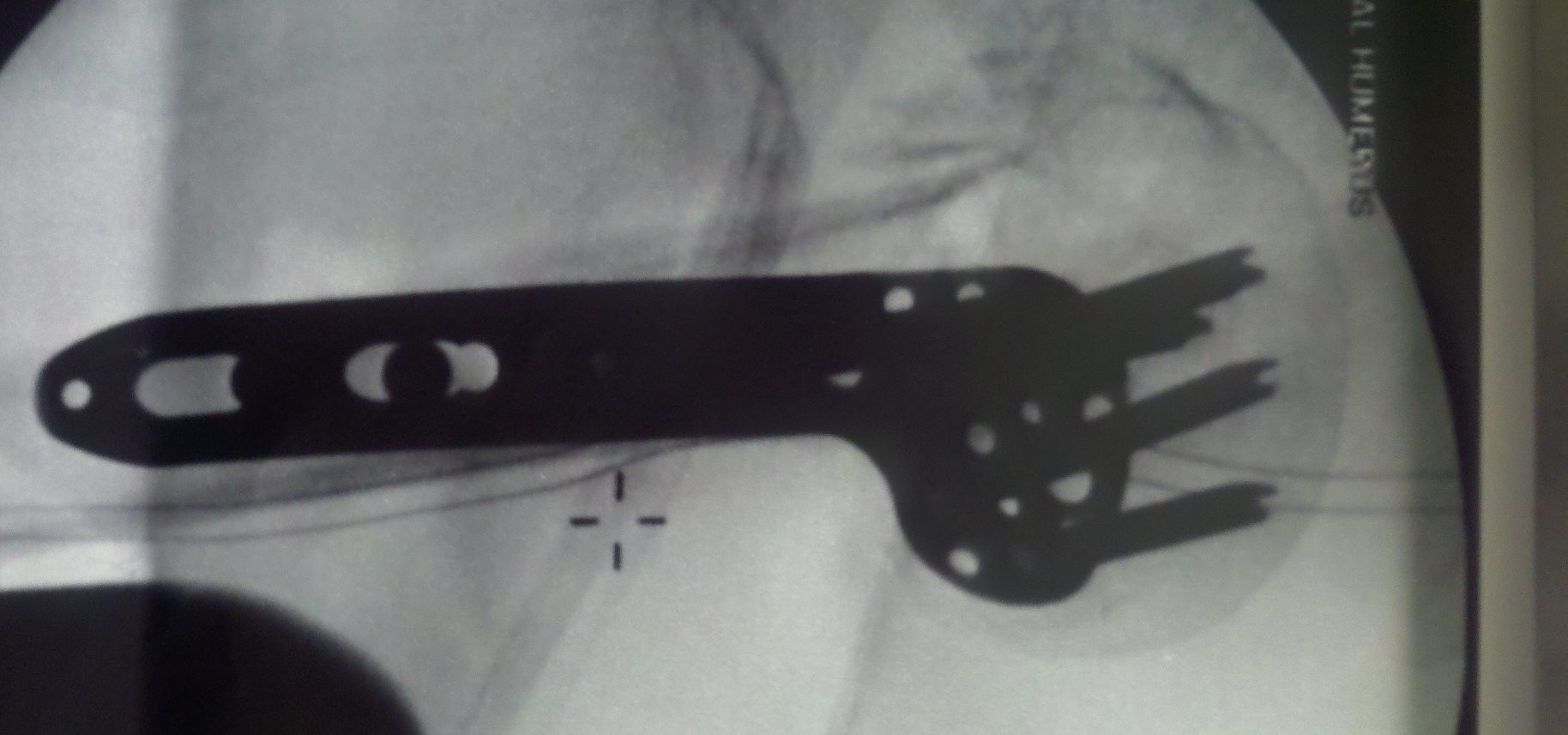 center of the humeral
center of the humeral
head in the subchondral abutment position;
- inferomedial screws:
- superiorly directed oblique locked screw in the inferomedial region of proximal fragment, may achieve more stable medial column
support and better maintenance of reduction;
- consider drill through the lateral cortex only, and then firmly inserting the depth gauge until the medial cortex is palpated;
- screw penetration is more likely if: (see considerations of screw insertion for hip fractures)
1) if screws are placed too close to articular surface
2) if articular surface is penetrated during drilling (may contribute to postop frx site instability and postop screw migration into joint);
3) if screws are inserted into the anterosuperior quadrant (should be avoided);
- bone grafting:
- Allogenic bone grafting for augmentation in two-part proximal humeral fracture fixation in a high-risk patient population
- references:
- The importance of medial support in locked plating of proximal humerus fractures
- Fracture displacement and screw cutout after open reduction and locked plate fixation of proximal humeral fractures [corrected].
- Screw Depth Sounding in Proximal Humerus Fractures to Avoid Iatrogenic Intra-articular Penetration
- The Position and Number of Screws Influence Screw Perforation of the Humeral Head in Modern Locking Plates: A Cadaver Study.
- Effect of screw placement on fixation in the humeral head
- Complications:
- A systematic review of locking plate fixation of proximal humerus fractures
- screw cutout and painful hardware:
- references:
- Treatment of proximal humerus fractures with locking plates: a systematic review
- Open reduction and internal fixation of proximal humerus fractures using a proximal humeral locked plate: a prospective multicenter analysis.
- Outcome analysis following removal of locking plate fixation of the proximal humerus.
- Treatment of proximal humerus fractures with locking plates: A systematic review
- Early Complications in Proximal Humerus Fractures (OTA Types 11) Treated With Locked Plates.
- Predicting failure after surgical fixation of proximal humerus fractures
- Injury to the axillary artery, a complication of fixation using a locking plate.
- postoperative pain and stiffness:
- referenences:
- Arthroscopy After Locked Plating of Proximal Humeral Fractures: Implant Removal, Capsular Release, and Intra-articular Findings
- Outcome analysis following removal of locking plate fixation of the proximal humerus.
- general references:
- Prognostic factors for unstable proximal humeral fractures treated with locking-plate fixation.
- Analysis of efficacy and failure in proximal humerus fractures treated with locking plates.
- Locked plating of 3- and 4-part proximal humerus fractures in older patients: the effect of initial fracture pattern on outcome.
- Fixed-angle Locked Plating of Two-, Three-, and Four- part Proximal Humerus Fractures
- Open reduction and internal fixation of proximal humeral fractures with use of the locking proximal humerus plate. Surgical technique.
- Open reduction and internal fixation of proximal humeral fractures with use of the locking proximal humerus plate.
- Technical tips for fixation of proximal humeral fractures in elderly patients
- Philos Locking plates in proximal humerus fractures –literature review
- Philos plate fixation for proximal humeral fractures
- The use of locking plates in proximal humeral fractures: Comparison of outcome by patient age and fracture pattern
- Internal fixation of proximal humeral fractures with locking proximal humeral plate (LPHP) in elderly patients with osteoporosis
- Current Concepts in the Treatment of Proximal Humeral Fractures
- Displaced proximal humeral fractures: an Indian experience with locking plates.
- Clinical Longer-Term Results After Internal Fixation of Proximal Humerus Fractures With a Locking Compression Plate (PHILOS).

 *
* 

- blade plate technique:
- in the report by Ring D, et al, the authors describe their technique for using of blade plates and autogenous
cancellous bone graft to repair ununited fractures of the proximal humerus in 25 patients;
- healing was documented in 23 of 25 patients (92%);
- objective and subjective instruments documented substantial functional improvement in patients with healed fractures;
- results were classified as good or excellent in 20 of 25 patients, and few complications were encountered;
- references:
- The use of a blade plate and autogenous cancellous bone graft in the treatment of ununited fractures of the proximal humerus
- Semitubular blade plate fixation in proximal humeral fractures: a biomechanical study in a cadaveric model..
- Semitubular blade plate for fixation in the proximal humerus.
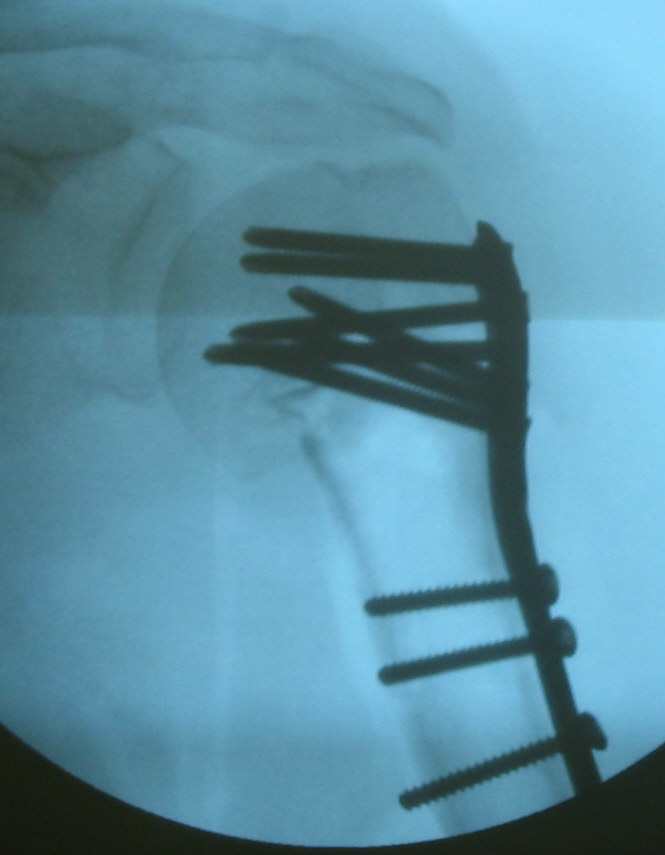
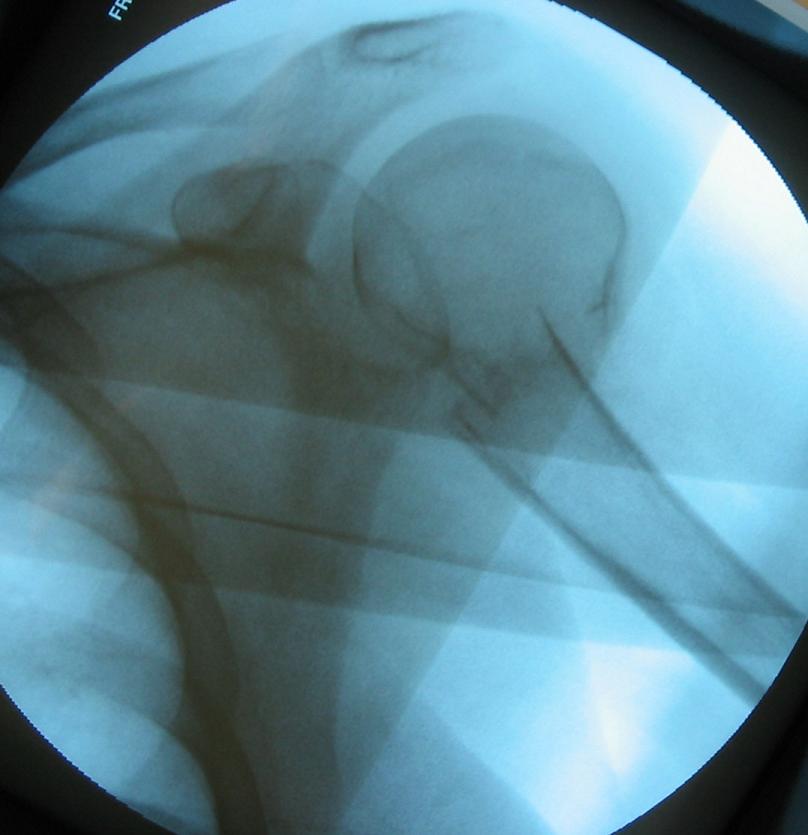
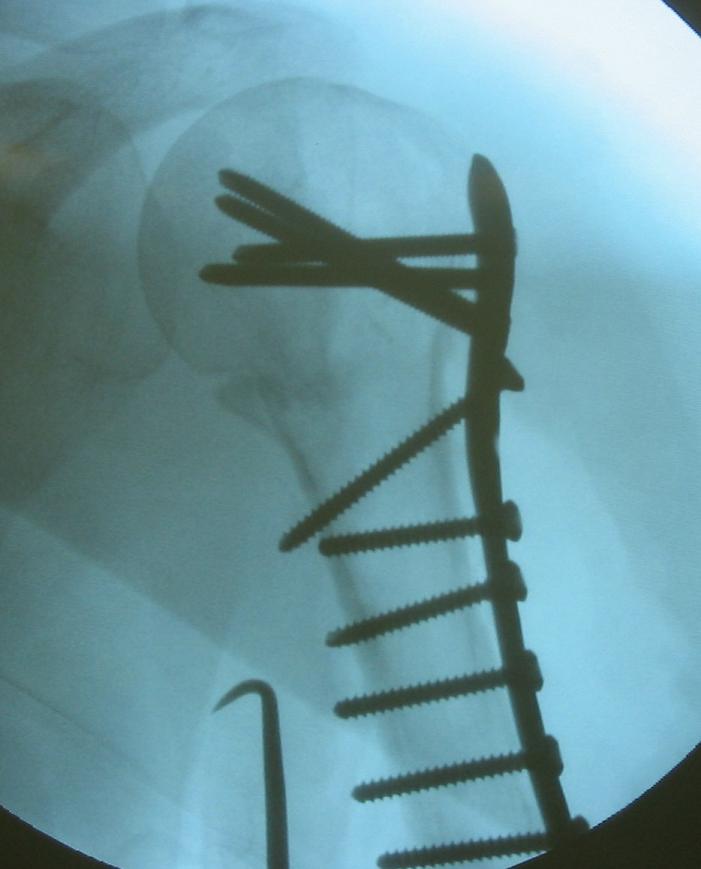
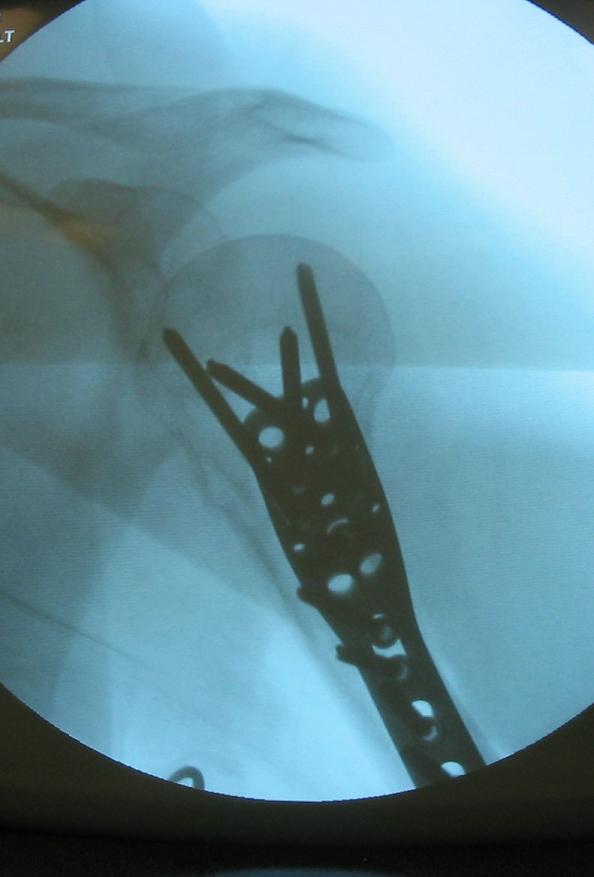
- 68-year-old female with a fracture dislocation of the proximal humerus surgical neck;
- because of the severe osteoporosis, the humeral shaft was pressed up and into the humeral head for added stability;
- a blade plate construct (using a semitubular plate) was applied into the lateral edge of the humeral head;
- the humeral head gradually reduced into the glenoid over 6 weeks;
 ***
*** 


 - T or L Plate:
- T or L Plate:
- implants include:
- T plate, L plate, standard 4.5 mm dynamic compression plate;
- 6.5 mm cancellous screw (both lag and fully threaded), & 4.5 mm cortical screws;
- DC plate may be placed laterally if there is sufficient room for two screws proximal to the frx;
- w/ oblique frxs of surgical neck fracture consider placing, a lag screw thru the plate across the fracture line;
- the main disadvantage of lateral plating is that the proximal screws often achieve a weak bite in the proximal humerus, which
can lead to hardware failure;
- in three and four part frx types, the 5 hole T or L plate may be chosen;
- typically the plate is placed on the anterio-lateral surface of the humerus, just anterior to the deltoid insertion;
- more lateral plate insertion is only possible if the deltoid insertion is stripped;
- anterior limb of T usually crosses long head of the biceps;
- this can be prevented by use of L plate, which allows fixation of proximal fragment w/ 2 large cancellous screws in proximal fragment
with two large cortical screws into the shaft;
- lag screws are inserted from proximal to distal;
- greater tuberosity fragment should be incorporated into fixation device or, alternatively, may be fixed w/ tension band wiring;
- as pointed out by Koval KJ, et al (1996), plate fixation is dependent on the quality of the patient's bone;
- in strong bone, plate fixation provides the strongest fixation, as compared to other methods;
- in osteopenic bone, there is a 3 fold decrease in fixation strength;
- in this case, percutaneous pinning provides better fixation;
- disadvantages:
- decreased fixation strength in osteoporotic bone (w/ possible loss of fixation), need for significant soft tissue dissection (which can lead to
avascular necrosis of frx fragments), subacromial impingement from the plate;
- reference:
- Surgical Neck Fractures of the Proximal Humerus: A Laboratory Evaluation of Ten Fixation Techniques.

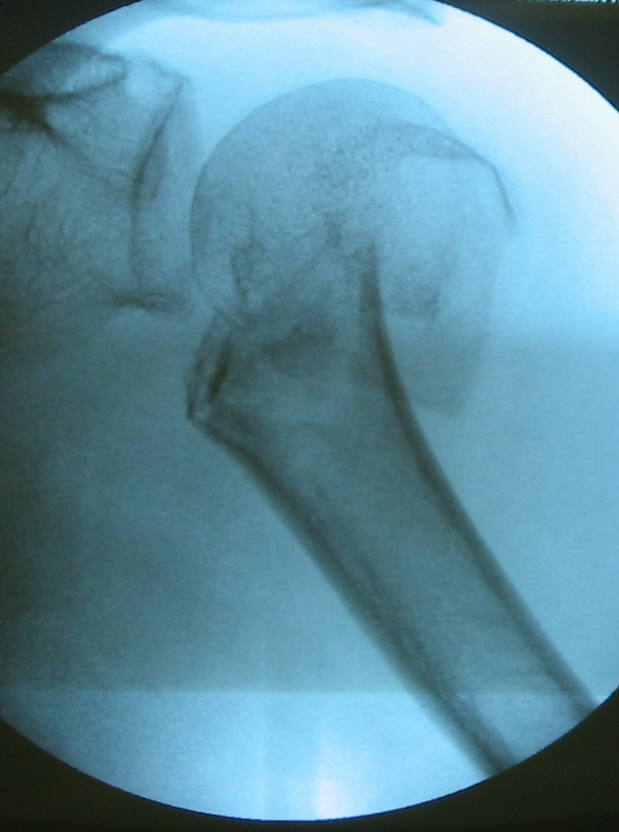
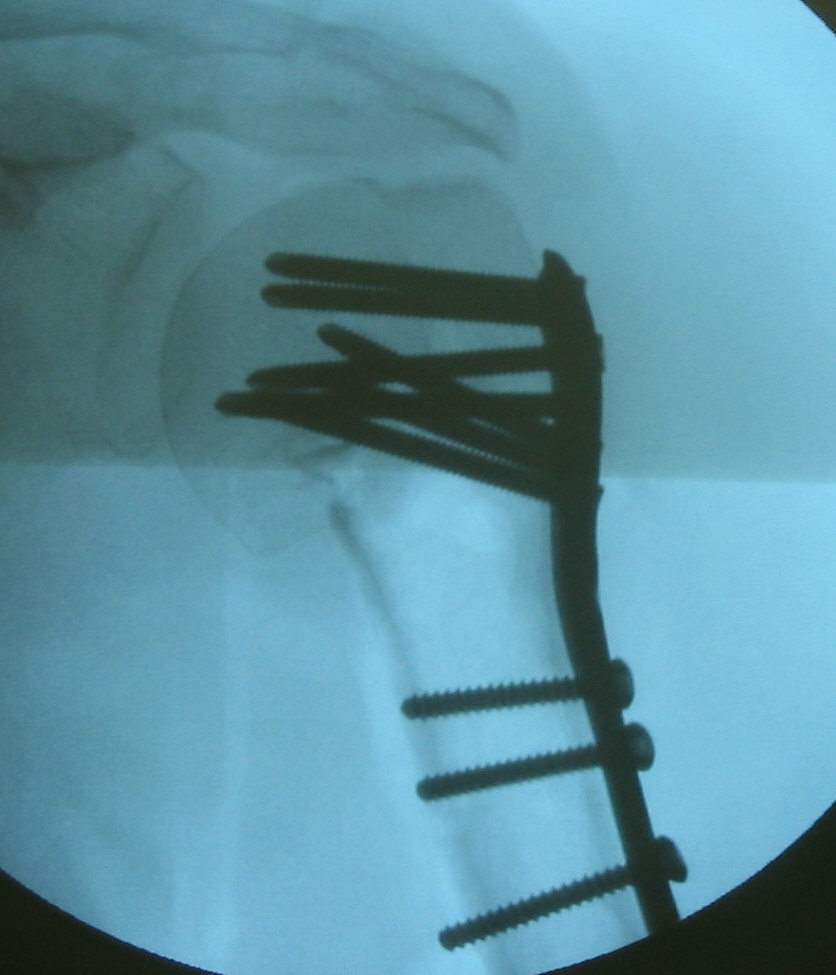
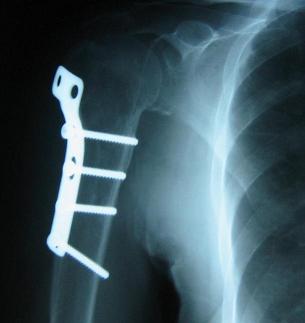
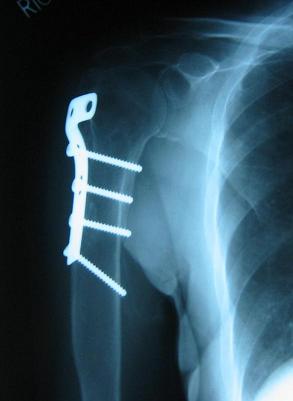
- in the following example, a 60-year-old female demonstrated a displaced proximal humerus frx with lateral displacement of the humeral head;
- treatment simply consisted of an antigluide plate, and at two years postop, there was a anatomic healing;

- Complications:
- hardware failure is a frequent complication w/ osteoporotic bone



Plate fixation of proximal humeral fractures.
Open reduction and internal fixation of three- and four-part fractures of the proximal humerus.