

- Discussion:
- frx occur as a result of a fall - from direct and indirect forces;
- occurs along lines between greater and less trochanters;
- theoretically extracapsular, however, it is not always possible to distinguish betwee intertroch and basilar femoral neck frx;
- extracapsular intertroch frx occur thru cancellous bone, which has an excellent blood supply - hence, heals well;
- that portion of the neck that is intracapsular has essentially no cambium layer in its fibrous covering to
participate in peripheral callus formation;
- therefore, healing in femoral neck area is dependent on endosteal union alone;
- forces acting on the hip joint
- classification
- basilar neck frx
- stable intertrochanteric frx
- unstable intertrochanteric frx
- lesser trochanteric frx
- reversed obliquity
- type-IV
- 4 part frx
- Non Operative Rx:
- even w/o treatment, frx usually stabilizes w/ in 8 wks & allows wt bearing in 12 weeks;
- however, marked varus of head & neck w/ assoc external rotation deformity usually results in a short leg gait & limp;
- Operative Treatment: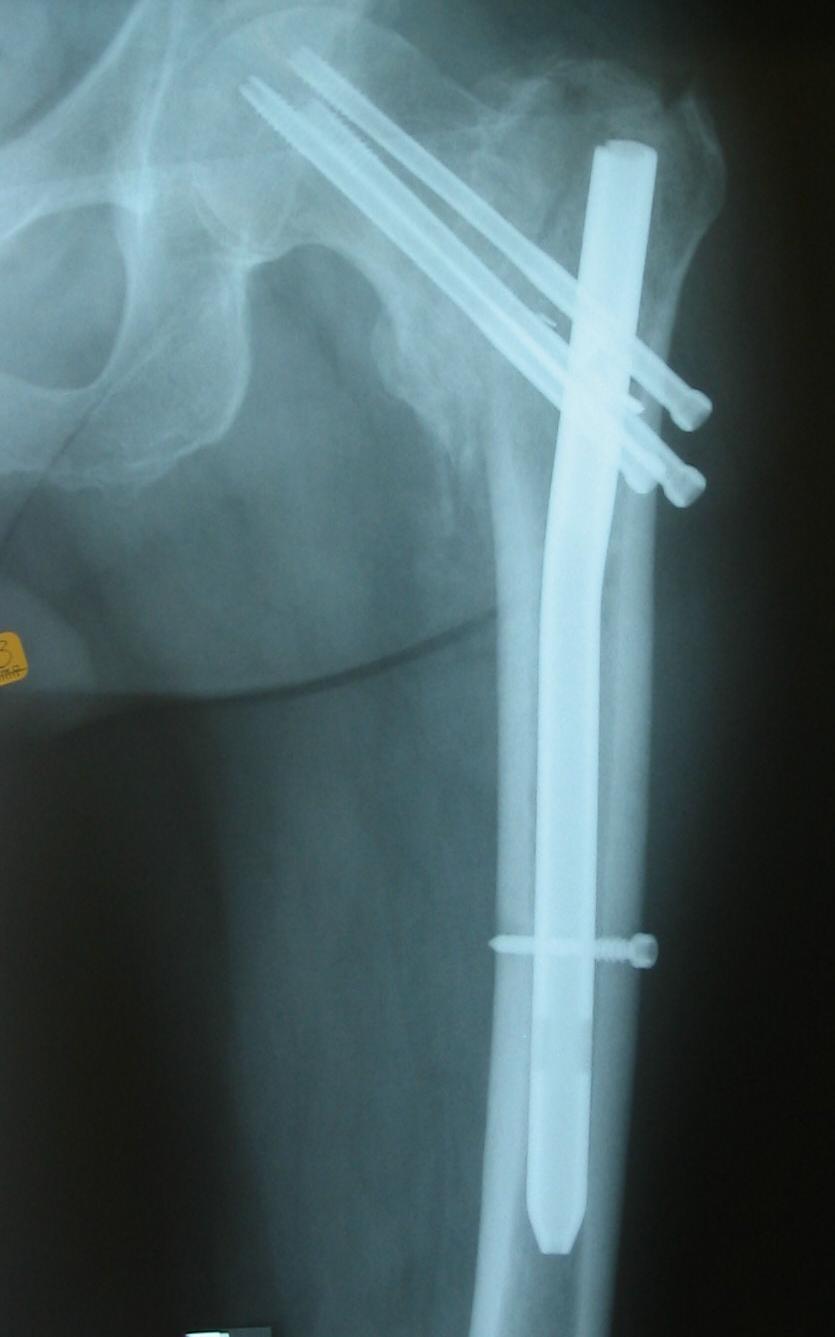
- surgical work up
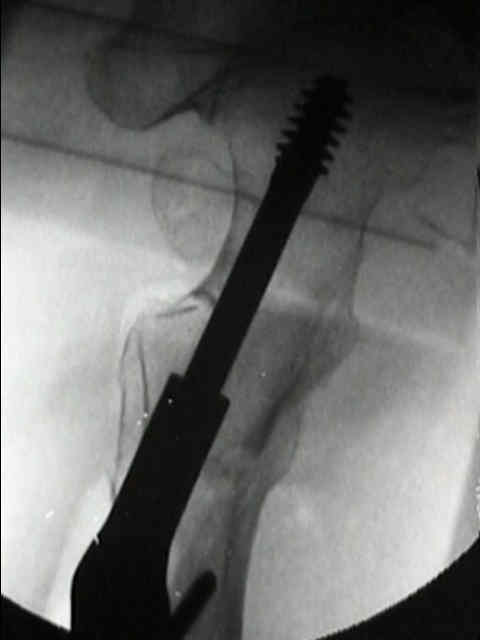
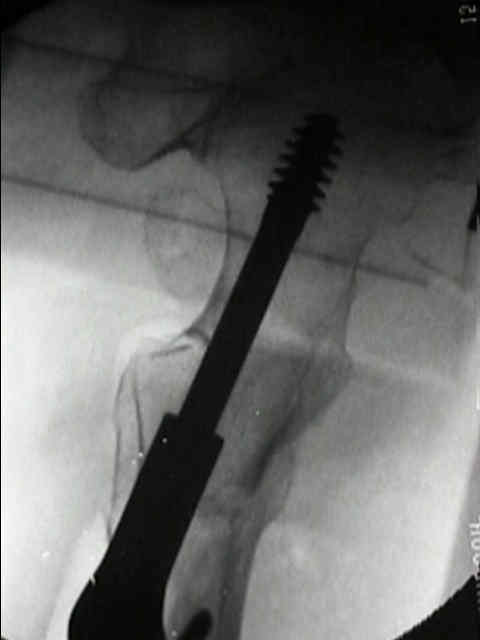
- sliding screw insertion technique
- intramedullary nail fixation
- hip arthroplasty
- references:
- Total hip arthroplasty for complications of intertrochanteric fracture. A technical note.
- Treatment of unstable intertroch /subtroch frx in elderly patients. Bipolar arthroplasty compared w/ IF.
- Total hip arthroplasty following failed internal fixation of hip fractures.
- Complications: Hardware Failure:
- Cementless modular hip arthroplasty as a salvage operation for failed internal fixation of trochanteric fractures in elderly patients.
- Hip arthroplasty for salvage of failed treatment of intertrochanteric hip fractures.
- Hip arthroplasty for failed internal fixation of intertrochanteric fractures
- Total hip arthroplasty for complications of proximal femoral fractures
- Salvage of failed internal fixation of intertrochanteric hip fractures
- Salvage procedures for failed compression hip screw fixation of intertrochanteric femoral fractures: analysis of 50 cases.
- [Conversion total hip replacement after failed internal fixation of intertrochantric fracture]
- Modular Femoral Component for Conversion of Previous Hip Surgery in Total Hip Arthroplasty
- Intertrochanteric femoral fractures. Mechanical failure after internal fixation.
- Avascular necrosis of the femoral head after intertrochanteric fractures.



 +
+ 

The fixation and prognosis of trochanteric fractures. A randomized prospective controlled trial.
Intertrochanteric femoral fractures. Mechanical failure after internal fixation.
Postoperative improvement of walking capacity in patients with trochanteric hip fracture: a prospective analysis 3 and 6 months after surgery.
Comminuted intertrochanteric fractures treated with a Leinbach prosthesis.
Trochanteric fractures. Mobility, complications, and mortality in 607 cases treated with the sliding-screw technique.
Analysis of six hundred and twenty-two intertrochanteric hip fractures.
External fixation of intertrochanteric fractures of the femur.
Postoperative weight-bearing after a fracture of the femoral neck or an intertrochanteric fracture.



- ender nails: (mentioned for historical purposes only);
- introduced in 1970;
- complications include: nails backing out of IM canal, perforation of nails thru femoral head, distal migration, and external rotational deformity at fracture site;
- references:
- The use of Ender's pins in extracapsular fractures of the hip.
- Ender nailing for peritrochanteric fractures of the femur. An analysis of indications, factors related to mechanical failure, and postoperative results.
- Unstable intertrochanteric fractures of the hip. Treatment with Ender pins compared with a compression hip-screw.
- A comparative analysis of Ender's-rod and compression screw and side plate fixation of intertrochanteric fractures of the hip.
- Complications of Ender-pin fixation in basicervical, intertrochanteric, and subtrochanteric fractures of the hip.