

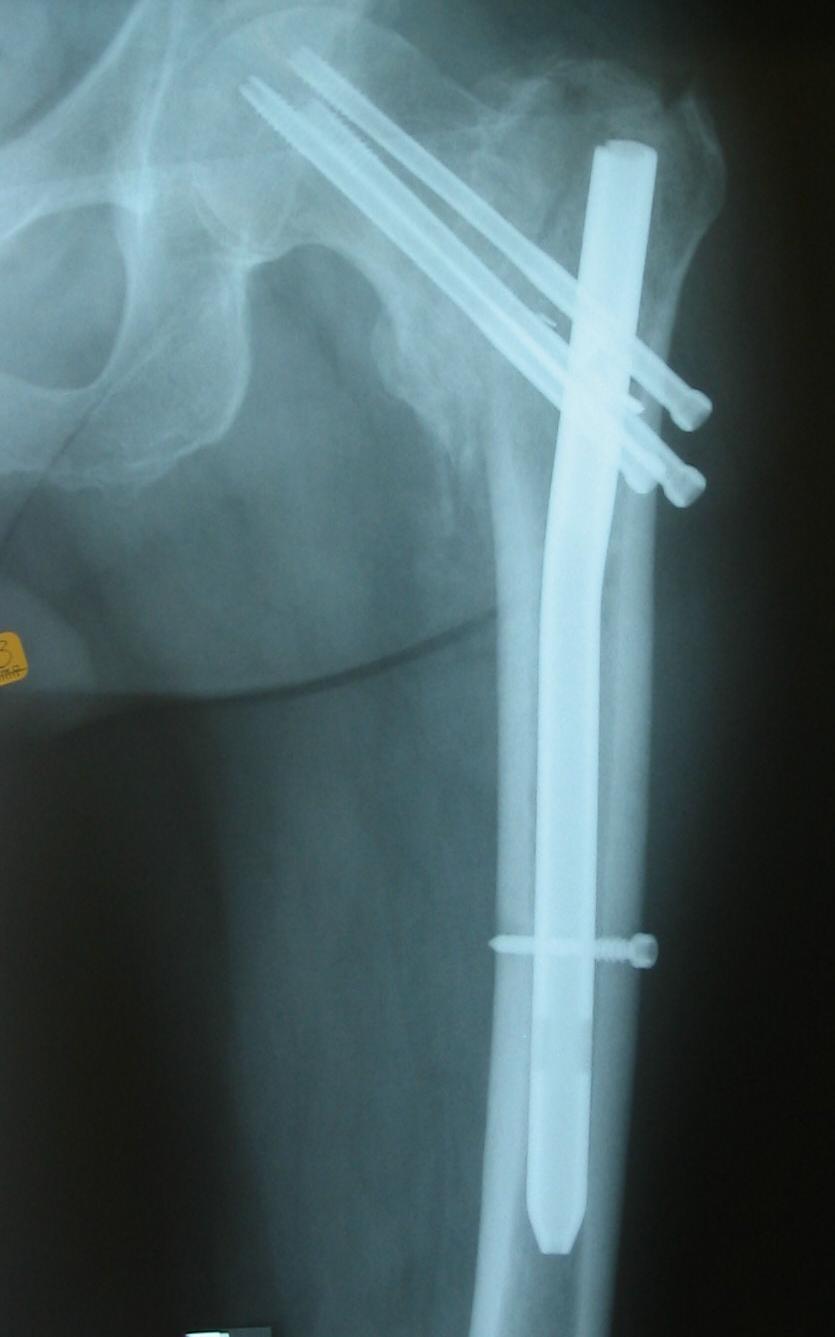
- a type of intramedullary device (designed for intertrochanteric and subtrochanteric fractures) which allows
controled sliding of the femoral head screw within the IM nail glidign hole;

- advantages of IM device:
- IM nail with interlocking reconstruction screws has better biomechanical advantage than sliding hip screw
and plate (forces acting on the hip joint);
- unstable intertrochanteric fractures:
- standard placement of sliding screw and plates often causes excessive medialization and/or
distraction at the fracture site where as insertion of sliding screw and plate at low angles (95
deg) will avoid medialization (and distraction) but will not allow sliding;
- in contrast, a properly inserted IM hip screw will block medialization of the fracture, and yet will allow
controlled sliding at fracture site;
- disadvantages of the IM device:
- thigh pain (attributed to use of 2 distal interlocking screws);
- need to obtain reduction prior to nail insertion;
- difficulty with optimizing placement of the femoral head screw,
- increased OR time;
- outcomes:
- in the study by Hardy, et al. (1988), nail was associated w/ less sliding than seen w/ compression hip screw
devices and had less limb shortening;
- references:
- Use of an intramedullary hip-screw compared with a compression hip-screw with a plate for intertrochanteric femoral fractures. A prospective, randomized study of one hundred patients.
- Functional recovery of elderly patients with surgically-treated intertrochanteric fractures: preliminary results of a randomised trial comparing the dynamic hip screw and proximal femoral nail techniques.
- Technical Considerations:
- surgical work up (see Synthes TFN)
- closed reduction
- reduction must be achieved either by closed or open means prior to nail insertion;
- failure to achieve reduction prior to nail insertion will complicate the nail insertion (one fragment may end up eccentrically opposed to
other) and wll make judgement of reduction on lateral view impossible (due to the nail and its targeting device);
- open reduction may initially be held with a single guide pin placed along the anterior margin of the fracture;
- far anterior insertion of the guide pin will not interfere with the nail insertion;
- intramedullary nailing technique
- entry position and guide wire insertion:
- w/ a trochanteric entry nail, start slightly medial to the specific tip of the greater trochanter;
- lateral entry will end up causing the fracture to reduce into varus (leads to non union and or malunion);
- lateral entry will end up causing a high lag-screw position in the femoral head (leads to cut out)
- posterior insertion will lead to anterior reconstruction bolt position (esp with females or with highly curved nails);
- technique tips:
- consider positioning the fracture table so that the affected leg can be briefly adducted to better present the
troachanter for the guide pin;
- remember as soon as the guide pin has been inserted, the leg needs to be put back into a slight abducted position (adduction
of the leg will cause a varus fracture reduction);
- with a difficult nail entry, have the OR nurse push on the opposite hip, inorder to increase hip adduction;
- references:
- Avoiding varus malreduction during cephalomedullary nailing of intertrochanteric hip fractures
- An anatomical study of the entry point in the greater trochanter for intramedullary nailing.
- Cephalomedullary nails: factors associated with impingement of the anterior cortex of the femur in a Hispanic population.
- reconstruction screw insertion in femoral head:
- same considerations for sliding hip screw;
- release traction after reconstruction screw is halfway across (allows better compression of fracture fragments
as recontruction bolt advances);
- value of helical blade:
- helical blade gives improved purchase in femoral head through radial compaction of cancellous bone around flanges of blade during insertion;
- bone of the femoral head with the helical blade is preserved compared to the bone loss that occurs with the drilling and
insertion of the standard sliding hip screw;
- hence, drill only enough bone to allow for advancement of the helical blade with moderate mallet blows.
- medial fragments:
- medial fragments may be secured w/ lag-screw tech if they can be captured w/o extensive dissection or periosteal stripping.
- biomechanical studies have shown increased stability of frx after fixation of large medial fragments;
- grafting of medial defects w/ autogenous bone should be done to promote early healing if medial comminution is present.
- reference: Screw fixation of the lesser trochanteric fragment.
- compression at frx site:
- although sliding reconstruction screw allows postop impaction at frx site, it is essential to obtain impacted reduction at time of surgery;
- this impacted position avoids excessive postop collapse that may exceed sliding capacity of the device;
- release traction, and use compression option if available;
- distal interlocking:
- Is distal locking with IMHN necessary in every pertrochanteric fracture?
- Distal unlocked proximal femoral intramedullary nailing for intertrochanteric femur fractures
- Failure of intertrochanteric nailing due to distal nail jamming.
- Pseudoaneurysm of a branch of the profunda femoris artery following distal locking of an intramedullary hip nail: an unusual anatomical location.
- A Biomechanical Comparison of Locked and Unlocked Long Cephalomedullary Nails in a Stable Intertrochanteric Fracture Model.
- Effect of distal interlock fixation in stable intertrochanteric fractures.
- postoperative care:
- Postoperative weight-bearing after a fracture of the femoral neck or an intertrochanteric fracture.
- complications:
- AVN of femoral head;
- Intertrochanteric femoral fractures. Mechanical failure after internal fixation. 
- Avascular necrosis of the femoral head after intertrochanteric fractures.
- hardware failure:
- Femoral Neck Fracture after Removal of the Compression Hip Screw from Healed Intertrochanteric Fractures
- vascular occlusion:
- Lower Extremity Bypass Graft Occlusion After Intramedullary Fixation of Intertrochanteric Hip Fracture on a Fracture Table
Use of an intramedullary hip-screw compared with a compression hip-screw with a plate for intertrochanteric femoral fractures. A prospective, randomized study of one hundred patients.
Intramedullary fixation of pertrochanteric hip fractures with the short AO-ASIF proximal femoral nail
The Holland nail: a universal implant for fractures of the proximal femur and the femoral shaft.
Cementless Calcar-Replacement Hemiarthroplasty Compared with Intramedullary Fixation of Unstable Intertrochanteric Fractures. A prospective, randomized study.
The Dynamics of Proximal Femoral Nails: A Clinical Comparison Between PFNA and Targon PF