

- See:
- Classification
- Singh index
- Unstable Intertrochanteric Fractures
- AP view (internal rotation);
- allows determination of frx obliquity & bone quality;
- if hip is in external rotation, greater troch rotates posteriorly & will overlie part of the fracture line;
- determine size, location, & comminution posterior frx fragments, which determines fracture (in)stability;
- in some cases the lesser trochanter will be fractured w/o comminution but more often there will be associated comminution which makes the frx unstable;
- Lateral:
- in some cases, an unstable frx pattern may be missed due to an inadequate lateral radiograph, which interferes w/ assessment of size postero-medial comminution and presence of coronal split in the greater troch (4 part frx);
- diagram of 4 part fracture: 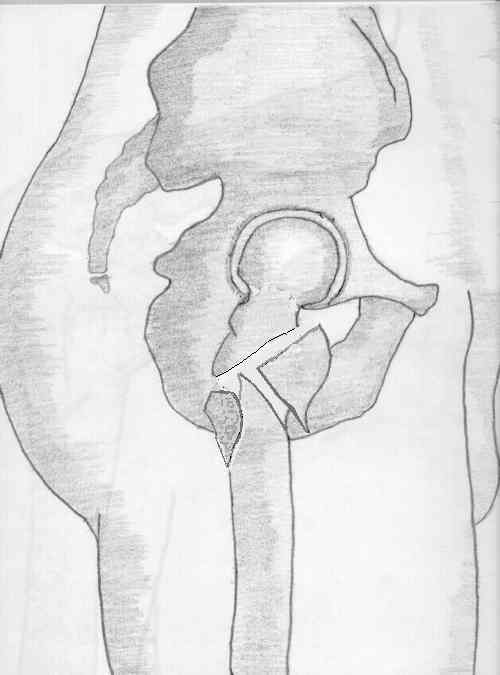
- 5Ps Hip Fracture: Pathologic Hip Fractures:
- ability of severely osteoporotic bone to bear substantial segment of load is impaired even when collapsible device is used properly.
- consider placing Sliding Screw more inferiorly in osteoporotic bone;
- purchase of cortical-bone screws thru side-plates may also be impaired in osteoporotic bone & may result in plate pulling away from shaft;
- this may be corrected by use of either longer plate & more screws;
- osteoporotic frxs must be protected w/ limited wt bearing postop;
- Fracture Geometry and Stability: (See Classification)
- w/ cortical instability on one side of frx owing to cortical overlap or destruction, frx tends to collapse in direction of instability;
- it is important prior to reduction to distinguish between Unstable and Stable Frx intertroch fractures