

- Discussion:
- type of tarsal coalition:
- calcaneonavicular bar is most common, followed by middle facet of the talocalcaneal joint;
- ossification occurs between 8 and 12 years;
- coalition between calcaneus & navicular is usually seen in pts between 8-12 years of age when cartilaginous coalition that results
from embryologic failure of tarsal segmentation undergoes ossification;
- Clinical Manifestations:
- rigid flatfoot with contracture of the peroneal tendons;
- symptoms occur because the ossification limits subtalar motion, which is required for normal walking;
- when foot is placed on ground in normal gait, sub-talar joint rotates externally to compensate for internal rotation of tibia on femur
w/ full extension at knee;
- if subtalar motion is restricted, navicular is displaced dorsally on talus & calcaneus is forced into valgus position
with each step;
- peroneus longus and brevis tendons adaptively shorten;
- when inversion of foot is attempted, the shortened peroneal tendons contract, pulling the foot into eversion;
- this contraction of the tendons also protects the subtalar area when it is painful;
- limited subtalar motion and peroneal tendon shortening contribute to rigid flatfoot;

- Radiographic Findings:
- oblique view:
- calcaneonavicular coalition is most clearly seen on the oblique view; (as described by Slomann in 1921);
- although visible on both AP and Lateral views, the coalition is much more difficult to recognize in these
projections;
- lateral view:
- often has signs suggestive of coalition:
- blunting of subtalar process, elongation of anteior calcaneal process, narrowing of posterior subtalar joint,
& talar beaking;
- talar beak was once considered sign of degenerative arthritis of the talonavicular joint & was an indication
to perform a triple arthrodesis;
- current trend is to disregard this finding and to perform a triple arthrodesis only if the joint itself
appears degenerative;
- MRI findings:
- perhaps most patients with calcaneonavicular coalition should have an MRI or CT scan to rule out concomitant
talocalcaneal coalition;



- Non Operative Treatment:
- symptomatic tarsal coalitions are initially be treated conservatively;
- immobilization followed by orthotic support is often sufficient;
- symptomatic lesions often are treated initially by immobilization for 3 to 6 weeks, followed by an orthosis;
- Indications for Surgery:
- if symptoms persist, then surgical intervention may be indicated;
- calcaneonavicular bars are amenable to resection, w/ most patients doing well;
- talar beaking is not considered absolute contraindication to bar resection;
- pts w/ degenerative arthritis in tarsal joints undergo arthrodesis;


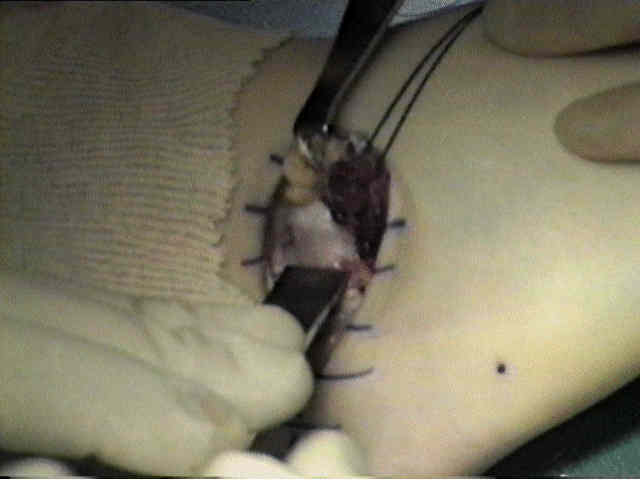
- Operative Technique: (bar resection);
- technique involves resection of bar and inter-position of EDB reduces the risk of refusion;
- use an oblique lateral incision (see Ollier incision)
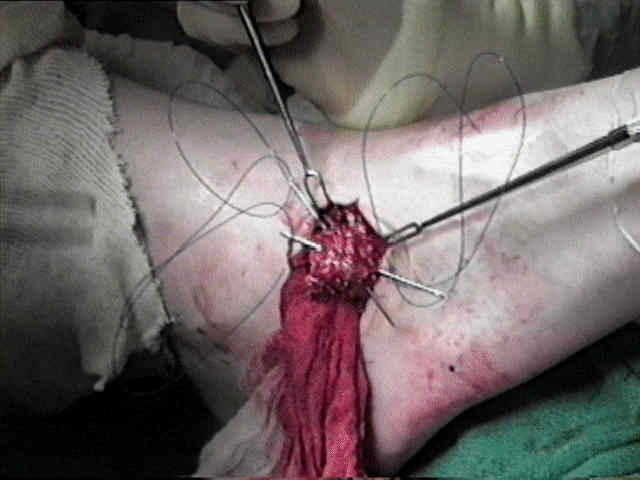
- EDB is freed from its insertion & reflected distally, w/care to preserve the nerve supply;
- care is taken not to injure the lateral branch of the deep peroneal nerve;
- coalition is located & talocalcaneal, talonavicular,
calcaneocuboid, & cuneonavicular joints are identified;
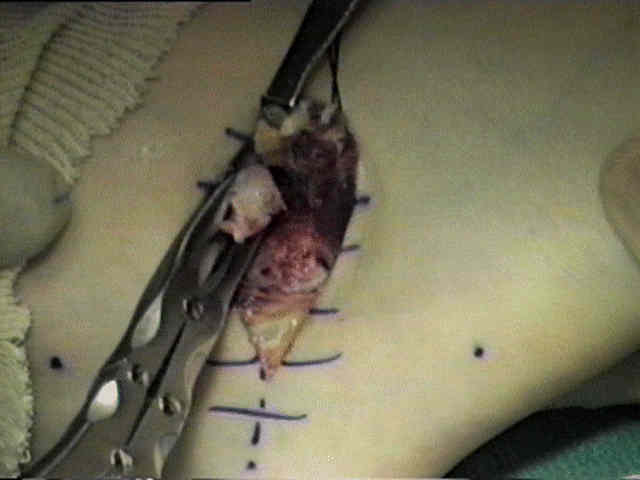
- rectangular section of the coalition is removed;
- to prevent recurrence, all cartilage must be removed from both calcaneus & navicular;
- note that plantar penetration of the bar may injure the calcaneo-navicular "spring" ligament;
- extensor digitorum brevis is then placed into the defect;
- an intraoperative radiograph is helpful to ensure that the resection is adequate;
- Post Op:
- pt wears below knee cast for 7-10 days, & begins subtalar motion;
- wt bearing is not allowed until the amount of subtalar motion reaches that obtained during the
operation - 3 to 4 weeks
Surgical reconstruction for calcaneonavicular coalition. Evaluation of function and gait.
Calcaneonavicular coalition treated by resection and interposition of the extensor digitorum brevis muscle.
Calcaneonavicular coalition resection with extensor digitorum brevis interposition in adults.