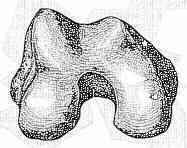
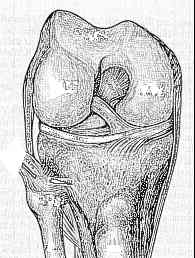
- Pertinent Surgical Anatomy
- Operative Treatment: Choice of Hardware:
- 95 deg. condylar blade plate:
- dynamic screw and side plate:
- condylar buttress plate:
- IM nails for supracondylar fractures:
- zickel nail:
- may be used for extra-articular transverse supracondylar fractures
- good for osteoporotic bone;
- Preoperative Planning:
- template for fracture fragments;
- must r/o a Hoffa extension (coronal plane fracture) in which case, a condylar buttress plate is required; (see classification);
- w/ a blade plate, the angulation of the screws in the plate (to avoid fracture lines on the other side) may be determined;
- determine anatomic axis from the uninjured knee;
- select implant;
- consent pt for ICBG;
- Surgical Strategy: (for intra-articular fractures)
- restoration of articular anatomy:
- restoration of articular surface w/ direct visualization of fracture using a limited medial para-patellar arthrotomy (keep skin incision
medial and distal inorder to avoid a narrow skin bridge) - see blood supply to the knee;
- after adequate exposure, femoral condyles are reduced & fixed w/ K wires;
- then definitively fix with large cancellous screws;
- use washers with poor bone stock;
- cancellous screws are placed anterior & posterior in condyles, allowing sufficient space between them for insertion of condylar blade plate;
- restoration of extra articular anatomy:
- simple bump: round bump under the frx site assists reduction of the supracondylar fracture by reversing the typical recurvatum deformity;
- restoration of ligamentous stability:
- once knee is stabilized, ligamentous injury about knee is assessed;
- before stabilization of fracture, it is difficult to determine extent ofinjury to the ligaments;
- medial instability is commonly present w/ supracondylar frxs;
- Positioning:
- supine, foley, sterile tournequet, hip bump, and operative knee elevated on towels (so that the opposite leg is not visualized when the flouro is obtained);
- flourotable w/ flouro on opposite side of table;
- ensure that pt is prepped and consented for ICBG;
- Frx Reduction:
- consider use of femoral distractor
- femoral condyles are reduced w/ K wires;
- 2 cannulated screws are inserted, one screw as anterior as possible and one screw placed as posteriorly as possible w/o going into the notch;
- hence, placement of these screws will allow sufficient space between them for subsequent insertion of the condylar blade plate or screw;
- due to the trapezoidal shape of the femoral condyles, which are narrower anteriorly than posteriorly, the cannulated screws should be 1 cm
short of the medial femoral cortex;
- following insertion of cancellous screws, the extra-articular portion of the fracture is reduced and stabilized