

- See:
- Rupture of FDP
- Flexor Tendon Repair
- Staged Tendon Reconstruction:
- Tendon Repair Technique:
- Zone I Injuries
- Zone II injuries
- Zone III injuries
- Zone IV and Zone V:
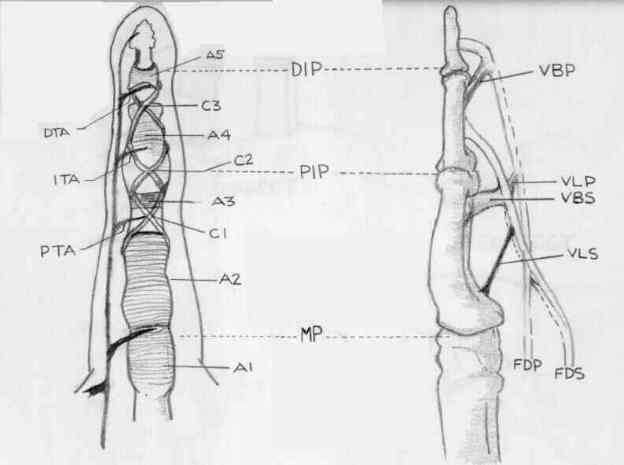
- Tendon Sheath Anatomy
- Discussion:
- skin laceration may not coincide with the point of tendon laceration
- primary repair is performed if the wound is clean;
- repair may be delayed seven to 21 days or even as long as six weeks after the original laceration;
- tendon is mobilized proximally, annular ligaments are maintained & tendon is advanced distally & sutured to distal stump by end to end
suture or by advancement if the distal stump is one cm long or less;
- advancement greater than one cm causes contracture;
- avoid lumbical plus finger:
- excessive advancement of FDP tendon to long, ring, or little fingers results in extension deficit of that finger;
- loss of flexion of the adjacent, uninjured digits is also noted;
- index finger is not generally affected by FDP tendon advancement in long, ring, & little
fingers because it usually exists as independent muscle belly;
- maximum tolerated advancement in the long, ring, and little fingers is 1 cm and is 1.5 cm in the index finger;
- Relative Contra-Indications for FDP Repair:
- rupture of previously repair FDP;
- elderly or non-compliant patient who will not tolerate prolonged rehabilitation;
- neglected zone II injury (this requires staged repair)
- arthritic DIP joint;
- A4 pulley rupture;
- Conversion to Superficialis Finger:
- hyper-extension deformity is prevented by tenodesis of FDP tendon;
- superficalis finger is fairly well tolerated;