

- Discussion:
- see flexor tendon repair
- see FDP lacerations: FDS and FDP
- almost all tendon injuries in zone 2 are due to lacerations;
- this is where 2 tendons enter fibro-osseuous tunnel at mid-palm level;
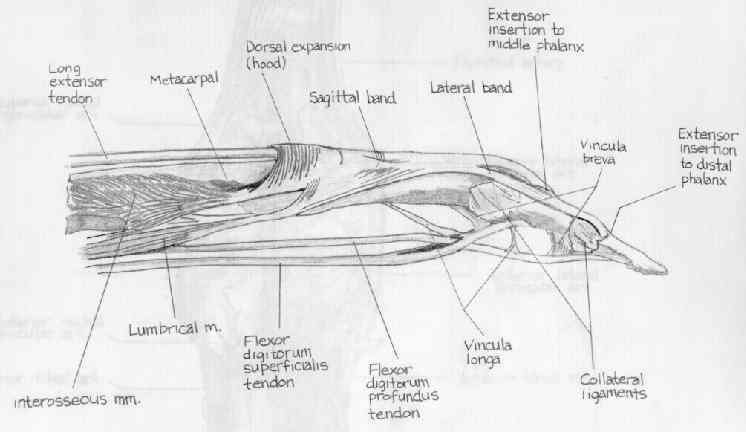
- once the FDS and FDP tendons enter flexor tendon sheath, the FDS separates into 2 segments, which pass around FDP tendon, and which
then reunite at Camper's chiasma (dorsal to the FDP);
- hences zone II lacerations will injure the FDP prior to injuring the two slips of the FDS tendon;
- note: that even in the best of hands, digital motion following Zone II injuries will be about 80% of the uninjured digits;
- evaulation:
- examiner should have the patient flex at the DIP joint to assess FDP function and at PIP joint, while holding adjacent digits in full
extension, to assess FDS function;
- digital nerve and arterial injuries are noted; (see nerve and artery repair)
- arterial injuries can be assessed by applying a "pulse oximeter" and then applying a digital allen's test;
- primary repair:
- primary repair of both tendons is performed only under ideal conditions;
- wound must be clean and well debrided of all crushed tissue;
- tendon sheath should be atleast partially intact;
- see:
- FDS laceration
- FDP laceration
- partial tendon lacerations
- delayed repair:
- even at 1 month following initial injury, end to end suture of both tendons is possible;
- neglected zone II injuries will require staged tendon grafting:
- controversies: should both flexor tendons be repaired?
- in zone II injuries in which both FDS and FDP are lacerated, both tendons should be repaired - expect up to 90% good or excellent results;
- the main complication of repair, is formation of adhesions to the flexor tendon sheaths;
- advantages of superficialis repair:
- repaired FDS increases digit strength;
- improved flexion at PIP joints
- preserves short vincula which provides blood supply to FDP and improves healing potential;
- acts as pulley for repaired profunda that provides improved excursion and strength;
- intact FDS prevents PIP hyperextension and DIP hyperflexion;
- ref: Work of Flexion Related to Different Suture Materials After FDP and FDS Tendon Repair in Zone II: A Biomechanical Study
- Exposure:
- see: phalangeal incisions:
- note: if both digital nerves are injured (which implies concomitant digital vessel injury) then it will be essential to carefully consider the incision so as not to create an avascular flap;
- digital wounds are extended both proximally and distally;
 - Management of Flexor Tendon Sheath:
- Management of Flexor Tendon Sheath:
- see: anatomy of sheath and pulley reconstruction;
- small portion of the fibroosseous canal may need to be opened, but as much of A2 and A4 pulleys as possible are left intact;
- it is not usually possible to close annular ligaments, once they are cut;
- in order to avoid impingment of flexor tendons with in flexor sheath, consider removal of a portion of flexor tendon sheath around tendon repair;
- one good option is to make a "Z" step cut incision into the pulley sheath;
- following the tendon repair, the pulley sheath is closed over the pulley, with assurance that the closure is not constrictive;
- another technique is to open sheath and then use a slip of extensor retinaculum in order to augment repair and to achieve a water tight closure;
- small longitudinal incisions can be made between the annular pulleys, which allows visualization of the flexor tendons;
- typically the surgeon will open the C1 or the C2 pulleys;
- the tendon repair will be completed in these annular windows;
- references:
- Effect of pulley integrity on excursions and work of flexion in healing flexor tendons
- A2 pulley incision or one slip of the superficialis improves flexor tendon repairs.
- Flexor tendon pulley V-Y plasty: an alternative to pulley venting or resection.
- "Venting" or partial lateral release of the A2 and A4 pulleys after repair of zone 2 flexor tendon injuries.
- Use of vein graft as a tendon sheath substitute following tendon repair: an innovative technique in tendon surgery.
- Results of primary tendon repair with closure of the tendon sheath.
- Flexor tendon repair and rehabilitation in zone II open sheath technique versus closed sheath technique.
- Biomechanical and histologic evaluation of tendon sheath management.
- Flexor sheath closure during delayed primary tendon repair
- Tendon Retreival:
- distal tendon edge:
- if fingers are flexed during the injury, the distal end of the tendon may retract 1 cm distal to the tendon sheath wound;
- DIP is flexed (and PIP if needed) to bring tendon edge into optimal position within the cruciate window;
- proximal tendon edge:
- Morris and Martin (1993)
- single pronged skin hook is carefully inserted into sheath, and at least one tendon edge is secured;
- withdrawl of the hook should retrieve both tendons;
- Sourmelis and McGrouther (1987);
- a small catheter is passed into the sheath and is delivered proximally into a small wound in the palm, just proximal to the A1 pulley;
- if the tendons have retracted proximal to the synovial sheath, the relative positions of the tendons must be restored;
- i.e., the FDP must pass from dorsal to volar through Camper's chiasma;
- catheter is sutured to both tendons 2 cm proximal to A1 pulley, which is then pulled distally to deliver tendons into synovial windon;
- tendon ends are held in place with 25 gauge needle inserted thru annular pulleys;
- if more than 1 cm of tendon edge can be exposed then the core suture can be inserted thru a single synovial window;
- references:
- A simple tendon retrieval method.
- A further tendon retrieval trick.
- The use of skin hooks and hypodermic needles in tendon surgery.
- Retrieval of the retracted flexor tendon.
- Retrieving tendon ends in zone II flexor tendon injuries.
- A simple, semirigid, and surgeon-friendly tendon retriever and flexor sheath dilator.
- The reversed Esmarch tourniquet technique for the retrieval of cut flexor tendons
- Tendon Repair: (tendon repair technique)
- consider use of the tenofix device;
- ref: Device for Zone-II Flexor Tendon Repair. A Multicenter, Randomized, Blinded, Clinical Trial.
- only on rare occassions do tendon edges require debridement;
- traumatizing the outer surface of the tendon with instruments may cause additional adhesions;
- instead, press cut end of tendon against against adjacent tissues / blunt end of forceps, and then pass suture;
- FDS tendon slips are repaired initially;
- when the laceration occurs near the FDS insertion, consider repairing both slips w/ figure of 8 sutures;
- avoid constriciton of the FDS tendon slips over the FDP repair (will inhibit gluiding):
- in report by Zhao C, et al (2002), authors examined effect of releasing 1 slip of FDS w/ FDP lacerations;
- after FDP repair the gliding resistance after modified Kessler repair increased 247% with FDS intact, 132% with one slip of
FDS present, and 103% with FDS entirely removed;
- references:
- Resection of the flexor digitorum superficialis reduces gliding resistance after zone II flexor digitorum profundus repair in vitro.
- Flexor Digitorum Superficialis Repair Outside the A2 Pulley After Zone II Laceration: Gliding and Bowstringing
- FDP is then repaired end to end using 4-O Ethibond suture w/ reinforcing peripheral sutures;
- core sutures are placed, using two separate double armed needles;
- ideally the core suture will contain at least 4 strands crossing the repair;
- core suture may be placed the primary window, but if exposure is not sufficient the surgeon can utilize the
more proximal or distal cruciate window (C1 and C2) w/ care taken to preserve the A3 pulley;
- this allows the the needle to move out of and into the tendon as the core stitch is being created;
- - management of repair impingement / indications for FDS sacrifice:
- when tendon repair requires sacrifice of pulleys
- when both tendons are lacerated & need to be immobilized at same level;
- as an alternative, consider staged tendon reconstruction:
- resection of one slip of the FDS to facilitate gluiding:
- in the report by Zhao C, et al (2002), authors examined effect of releasing 1 slip of FDS w/ FDP lacerations;
- after FDP repair the gliding resistance after modified Kessler repair increased 247% with FDS intact, 132% with one slip of FDS present, and 103% with FDS entirely removed;
- references:
- Resection of the flexor digitorum superficialis reduces gliding resistance after zone II flexor digitorum profundus repair in vitro.
- Pulley plasty versus resection of one slip of the flexor digitorum superficialis after repair of both flexor tendons in zone II: a biomechanical study.
- Impact of flexor digitorum superficialis on gliding function of the flexor digitorum profundus according to regions in zone II.
- Flexor sheath closure during delayed primary tendon repair
- “Venting” or partial lateral release of the A2 and A4 pulleys after repair of zone 2 flexor tendon injuries
- Tendon Sheath Repair: (see tendon sheath reconstruction)
- prior to extending digit, the sheath is closed w/ a running 6-0 monofilament;
- following tendon sheath repair, the digit is extended which delivers the tendon repair site distally;
- cautions:
- adequate tendon sheath repair is not only necessary to prevent bowstringing but it is also important to prevent flexion contractures;
- Post Operative Care
Strength and functional recovery following repair of flexor digitorum superficialis in zone 2.
Factors affecting results after flexor tendon repair in zone II: a multivariate prospective analysis.
Results of zone I and zone II flexor tendon repairs in children.
An unusual role of the vinculum after complete laceration of the flexor tendons.
Results of zone II flexor tendon lacerations in civilians treated by the Washington regimen.
The biomechanical analysis of a tendon fixation device for flexor tendon repair
Flexor Tendon Injuries
Original Text by Clifford R. Wheeless, III, MD.
Last updated by Clifford R. Wheeless, III, MD on Sunday, April 26, 2015 4:03 pm