

- See:

- Carpal Instability
- Ligaments of the Wrist
- Discussion:
- perilunate dislocation pattern provides a whole spectrum of wrist sprains, fractures, dislocations;
- types of perilunate dislocations (in order of frequency):
- transscaphoid-perilunate
- perilunar
- transscaphoid-trans-capitate-perilunar
- transradial-styloid
- Mechanism:
- carpal dislocations result from hyperdorsiflexion;
- severe ligament injury is necessary to tear the distal row from the lunate to produce perilunate dislocation;
- sequence of injury:
- this injury pattern usually begins radially & destabilizes thru body of scaphoid (w/ frx) or thru scapholunate interval (w/ dissociation);
- scaphoid bridges the proximal and distal carpal rows;
- w/ dislocation between these rows, the scaphoid must either rotate or fracture
- this produces a perilunate dislocation, which may cause: trans-sccaphoid perilunate dislocation:
- distal half of scaphoid & remaining carpus dislocate around lunate;
- force is transmitted ulnarly thru the space of Poirier (between lunate and capitate);
- next force transmission disrupts the luno-triquetral articulation;
- as a manifestation of the most severe form of the injury, the lunate may be dislocated into the carpal tunnel;
- transradial styloid perilunate dislocation:
- frx of radial styloid w/ dislocation of it & remaining carpus around lunate;
- further destabilization passes distal to lunate, either thru space of Poirier or thru capitate (transcapitate frx), & then ulnar to lunate, either through hamate & triquetrum or thru lunotriquetral interval;
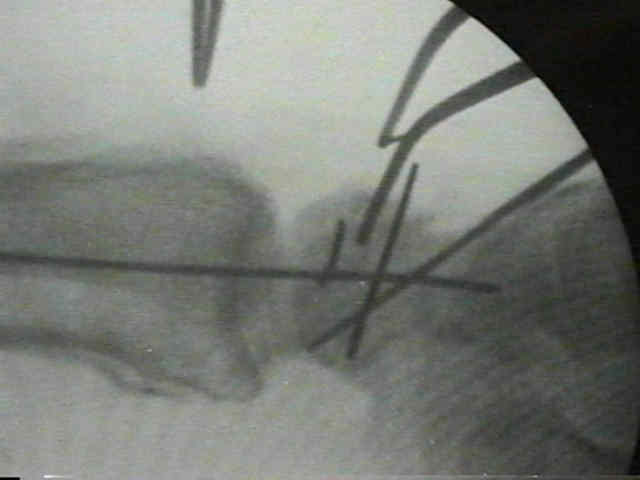
- Radiographs:
- lateral radiographs will reveal loss of co-linearity between the capitate, lunate, and radius;
- typically the captitate is located dorsal to the lunate and is aligned with the radius;



- Components of Perilunate Dislocation:
- includes dorsal dislocation of distal row, scaphoid, and triquetrum;
- lunate:
- vascularity of the lunate
- lunate is usually subluxated and angulated palmarly but still is located in the lunate fossa of the radius;
- w/ more severe injury lunate may be dislocated into the carpal canal, or if strong, short radiolunate and ulnolunate ligamens are torn, it may be displaced free fragment;
- lunate dislocation is considered the last stage of perilunate dislocation;
- example of lunate dislocation:


- capitate:
- capitate fragment is frequently turned 180 deg so that its articular surface faces cancellous surface of major capitate fragment;
- scaphoid & capitate fragments are devascularized by displacement;
- space of poirier:
- disruption occurs at scapholunate area & progresses into space of Poirier and then thru the lunotriquetral space;
- rent develops during dorsal dislocations, and it is thru Space of Poirier interval that the lunate displaces into the carpal canal;
- misc:
- DISI:
- DISI collapse pattern, occurs because stabilizing influence of scaphoid is inital component of dislocation;
- VISI:
- destabilization may begin ulnarly w/ a lunotriquetral dissociation;
- if lunate remains attached to scaphoid VISI will develop;
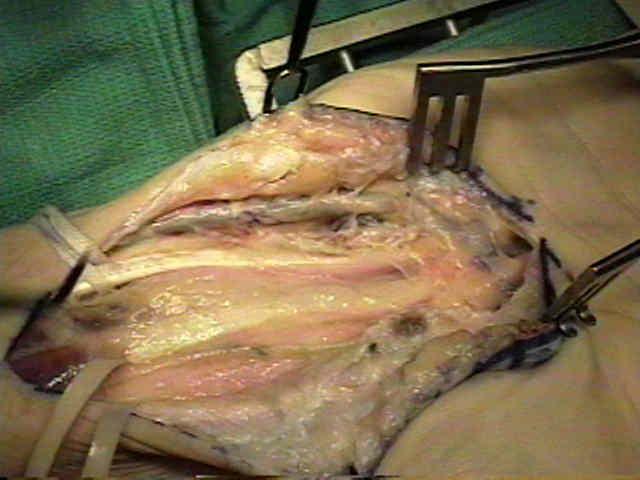
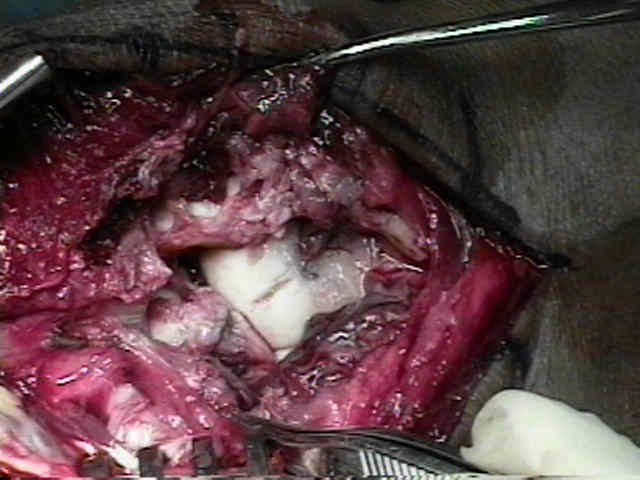
- Surgical Treatment:
- delineate between those dislocations which easily reduce w/ close reduction & those that are irreducible or unstable;
- in the later group, interposed capsule may be preventing the reduction;
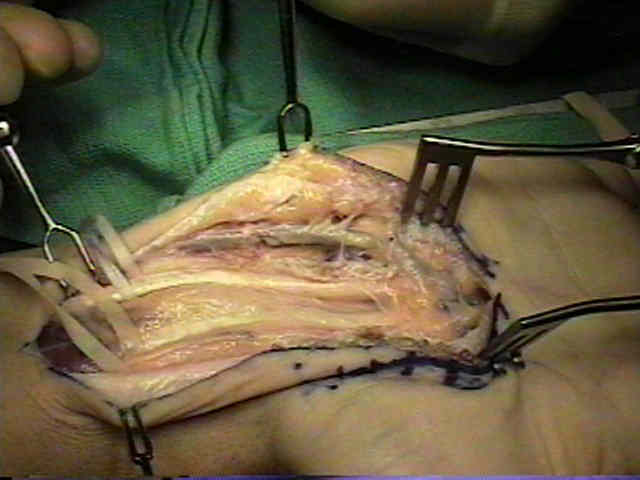
- palmar approach is typically needed to repair the rent in the volar capsule at the lunocapitate joint as well as carpal tunnel release;
- dorsal approach is required for scaphoid fracture fixation or repair the torn scapholunate interosseous ligament;
- note that one of the essential goals of treatment is to reduce the scapholunate gap (inaddition of volar ligament repair);
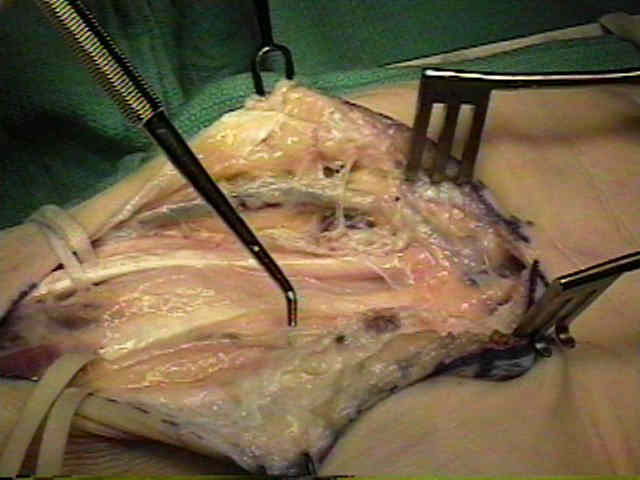
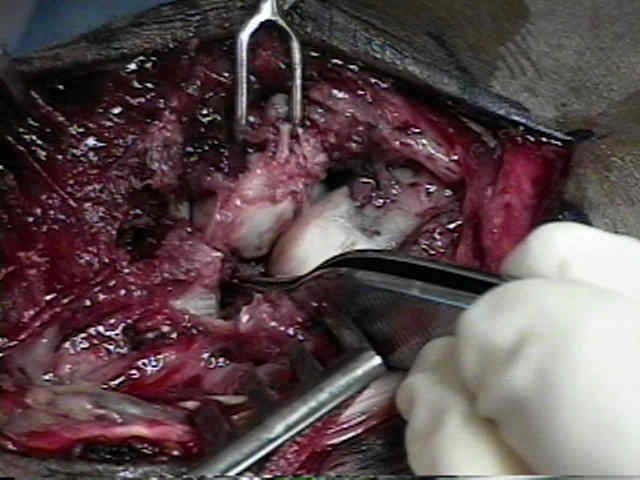
- volar approach:
- not all surgeons use a volar approach (unless a scaphoid fracture is present);
- in the case of a scaphoid fracture, the volar approach is devoted to fixing the fracture;
- if there are neurovascular problems, a volar approach allows release of carpal tunnel;
- combined w/ dorsal approach, this allows both intra articular & extra-articular damage to be assessed and treated adequately;
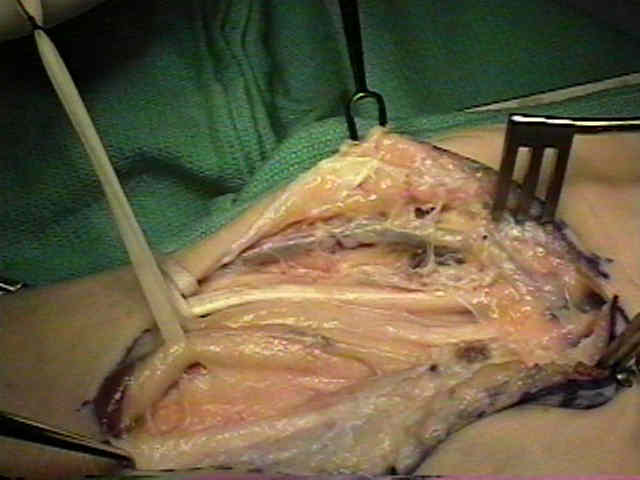
- volar approach allows better reduction of the lunate and repair of the volar capsule;
- may be opened, either along its attachments to radial rim or thru the constant rent in the space of poirier;
- reference:
- The palmar radiocarpal ligaments: A study of adult and fetal human wrist ligaments.
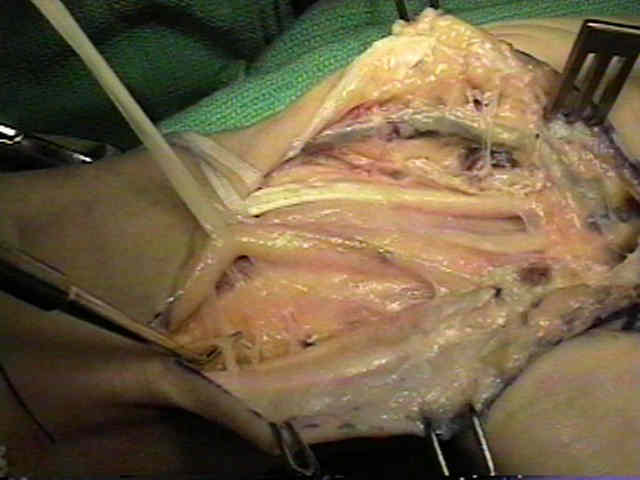
- dorsal approach:
- some surgeons rely on the dorsal approach alone for surgical fixation of perilunate dislocations;
- in the study by Cooney, et al (1987), 18 of 21 patients who underwent a dorsal approach had a satisfactory outcome;
- patient is supine w/ wrist slightly flexed & placed on arm board;
- perform a provisional reduction before the incision is made;
- incision:
- Z or S shaped incision from base of second metacarpal over wrist to distal forearm is suggested for good healthy skin;
- alternatively, make a straight midline longitudinal one in line w/ third metacarpal and into the distal forearm;
- the incision will be made thru the 3rd compartment;
- this passes safely between the dorsal sensory branches of the ulnar nerve medially, and ofthe radial nerve laterally;
- ref: Difficult wrist fractures. Perilunate fracture-dislocations of the wrist.
- extensor retinaculum:
- extensor retinaculum between the 3rd and 4th extensor compartments is reflected off of wrist capsule w/ care to avoid any damage to capsule itself;
- EPL is mobilized out of its sheath and is reflected radially;
- subperiosteally elevate the fourth compartment, w/o violating the tendon sheath;
- place Homan retractors on either side of the radius;
- capsular incision:
- longitudinally incise thru the dorsal capsule in line w/ Lister's tubercle, and then elevate the wrist capsule off of the dorsal rim of the distal radius including the dorsal radiotriquetral ligament;
- preserve radiotriquetral ligament;
- need to remove loose fragments
- dorsal capsule is usually opened along its origins from dorsal rim, & longitudianlly in space between 2nd & 4th extensor compartments;
- it is easier to examine cartilage surfaces & intra articular fragments thru the dorsal approach;
- note that some surgeons elect to fix the scaphoid fracture (if one is present) through the dorsal incision;
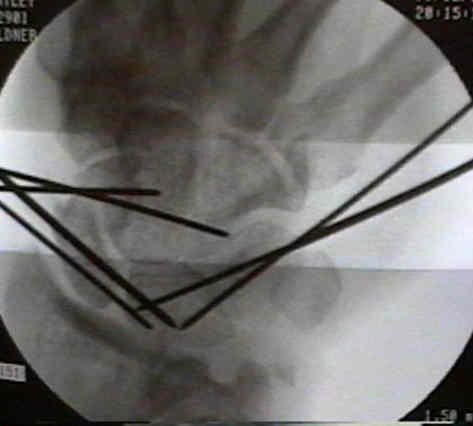
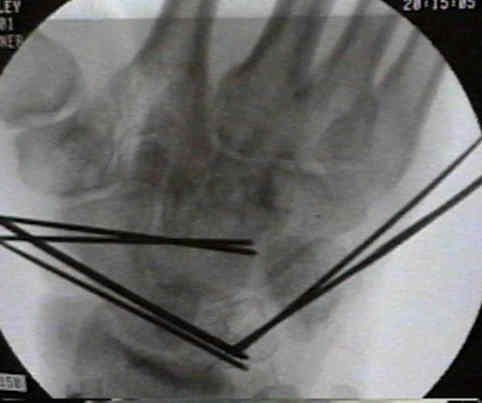
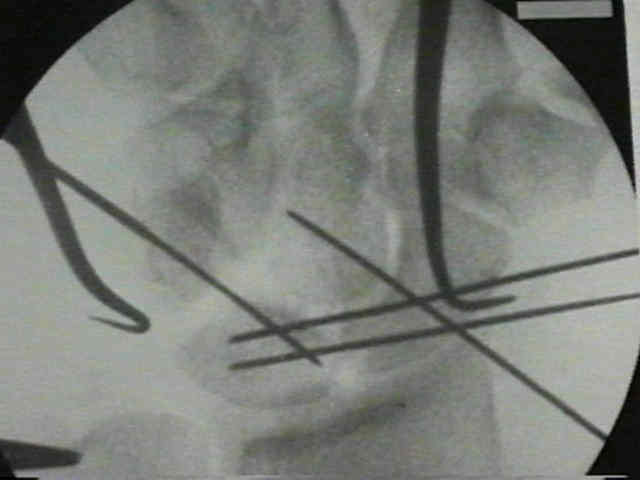
- K wire fixation:
- following either open or closed reduction, K wire fixation will be required;
- the usual statedgy includes:
- ORIF of scaphoid fracture, if one is present (see trans-scaphoid perilunate dislocation);
- temporary lunate fixation to the radius (w/ care to take the lunate out of dorsiflexion);
- alternatively insert a K wire into the lunate which then can be used as a joystick;
- capitolunate angle should be held at neutral or slight flexion;
- scapholunate fixation;
- before the scapho-lunate joint is pinned, pass the ligamentous repair sutures, but do not tie them together until all of the pins have been inserted and the reduction is optimal;
- once K wire fixation has been achieved, consider repairing the scapholunate interosseous ligament with a bone anchor, and then augmenting the repair with a dorsal capsulodesis;
- scapho-capitate fixation;
- w/ an optimal reduction, the lunate should cover the head of the capitate;
- triquetral-lunate fixation;
- Post Op:
- patients should understand clinical improvement takes upto one year;
- Complications:
- secondary carpal collapse;
- scapholunate dissociation;
- lunotriquetral dissociation;
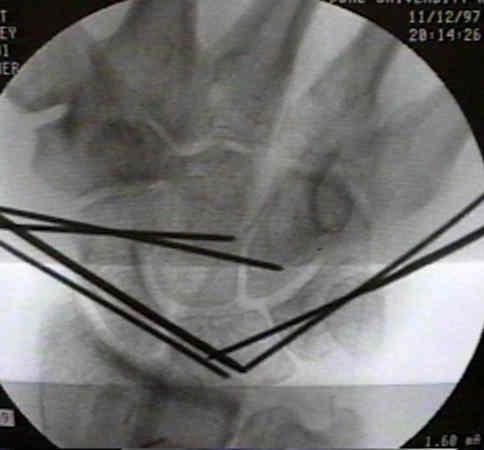
- Case Example:
- 50-year-old male who was assaulted, sustaining a lunate dislocation;

Problem Fractures of the Hand and Wrist--Symposium: Difficult Wrist Fractures: Perilunate Fracture-Dislocations of the Wrist.
Current Concepts Review. Carpal Instability.
Chronic capitolunate instability
Dislocations of the lunate with and without fracture of the scaphoid.
Carpometacarpal dislocations. Long-term follow-up.
Open reduction of carpal dislocations: indications and operative techniques.
Transient vascular compromise of the lunate after fracture-dislocation or dislocation of the carpus.
Difficult wrist fractures. Perilunate fracture-dislocations of the wrist.
Median-nerve neuropathy associated with chronic anterior dislocation of the lunate.
Posttraumatic ulnar translation of the carpus.
Perilunate dislocations and fracture-dislocations: a multicenter study.
Perilunate dislocation and fracture dislocation: a critical analysis of the volar dorsal approach.
Radiocarpal Dislocations: Classification and Proposal for Treatment. A Review of Twenty-seven Cases
Perilunate Fracture–Dislocations of the Wrist: Comparison of Temporary Screw Versus K-Wire Fixation.