

- Position:
- place patient in a beach chair position w/ torso flexed 45 deg and the knees flexed to 30 deg;
- move patient to the edge of the table (operative side), and use a McConnel positioner to prevent the patient from failing off the table;
- patient must lie far enough off the side of table to that the shoulder can be fully extended, externally rotated w/o interference - some
adduction should also be possible;
- note that improper positioning may complicate operative dislocation and may interfere with access to the medullary canal during
broaching, and stem insertion which risks humeral fracture;
- place a folded towel under the spine and ipsilateral scapula;
- use a McConnel upper limb positioner or a Mayo stand to hold the arm during the case;
- methods to prevent infection:
- OR lights:
- position the OR lights prior to prepping;
- there is some evidence that "sterile" OR light handles are a common source of contaminant during surgery, and ideally
these should not be touched during the case;
- Extended Deltopectoral Approach 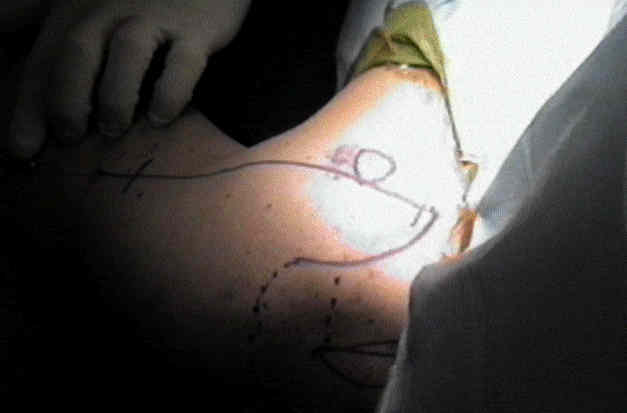
- Deep Exposure: (subscapularis and anterior capsule)
- positioning arm in adduction and external rotation may reduce risk to axillary and musculocutaneous nerves;
- this position may also place the axillary artery under tension (tension against the edge of the pectoris minor), and the
complication of thrombosis may especially high in elderly patients;
- ref: Axillary Artery Thrombosis After Humeral Resurfacing Arthroplasty
- identification of axillary nerve:
- volar aspect of the index finger palpates the nerve proximal to the quadrilateral space;
- a spiked homan is placed above the coracoid and is levered to provide superior retraction;
- the anterior Charnley (or Warren retractor) is placed in the subpectoral space;
- transection and mobilization of subscapularis: (see subscapularis anatomy)
- check for Loose Bodies:
- inspect the subscapularis fossa, the subcoracoid recess, the posterior axillary recess, and the bicipital groove for loose bodies
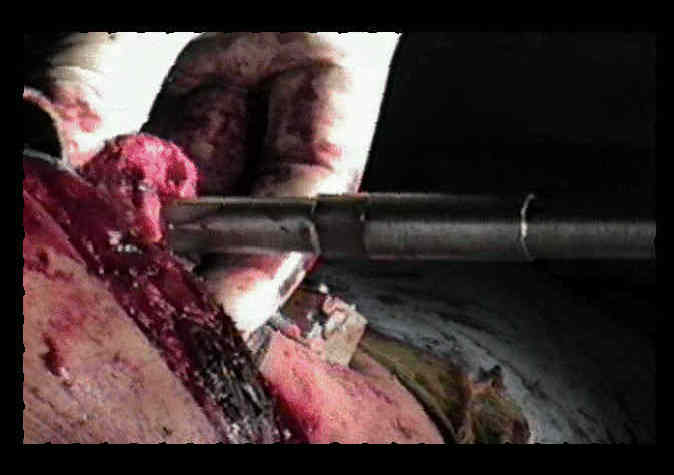
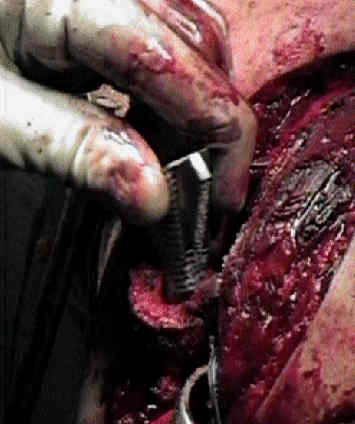
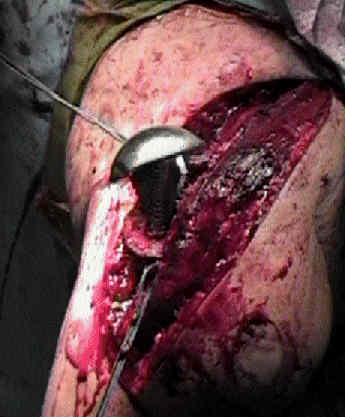
- Preparation of Humerus and Component Insertion:
- Glenoid Component:
- indications are controversial;
- this needs to be performed prior to insertion of the humeral component;
- a blunt homan or a "hip skid" retractor is placed in front of the proximal humerus and behind the posterior
glenoid in order to provide full exposure of the glenoid;
- careful not to excessively torque on the homan because this can cause greater tuberosity fracture;
- if exposure is not adequate consider sequential release of the posterior capsule off of the posterior glenoid rim;
- w/ hemiarthroplasty, make sure that the glenoid is concentric with respect to the humeral head;
- if a biconcave reamer is used then consider use of hemispherical reamers to convert the glenoid to a concentric surface;


- Wound Closure:
- it is essential to obtain a tight closure of the subscapularis tendon, since anterior instability often results from avulsion of the tendon at the repair site;
- for more secure repair, the subscapularis tendon can be sutured to the coracohumeral ligament (this closes down the rotator interval);
- carefully document the amount of external rotation that is possible without tension after subscapularis tension, and do not allow the
patient to externally rotate beyond this until six weeks post op;
- ref: Loss of subscapularis function after total shoulder replacement: a seldom recognized problem
- if the procedure has required osteotomy of the tuberosities, then ensure that they have been clear of scar tissue so that they can be approximated
around the prosthesis and the humeral shaft;
- if necessary, use a rongeur to thin out the tuberosity fragments if necessary;
- reduce the humeral head into the glenoid;
- pile bone graft along the transected edge of the proximal humerus, and then
- the tuberosity fragments are initially held together w/ a large towel clip;
- repair the tuberosities to each other, to the fin, and the humeral shaft;
- tuberosities are positioned so that RC insertions are below the prosthestic head (allows prosthetic head to mimic natural cam effect)
- remember the goal is to achieve fixation of the tuberosities to the humeral shaft rather than the tuberosities to the metal fin;
- always apply bone graft if gaps are present;
- biceps tendon is released from the supra-glenoid notch (if it hasn't been released already), and then is tenodesed to the tuberosities
Original Text by Clifford R. Wheeless, III, MD.
Last updated by Clifford R. Wheeless, III, MD on Monday, May 27, 2013 4:58 pm