

- Discussion: 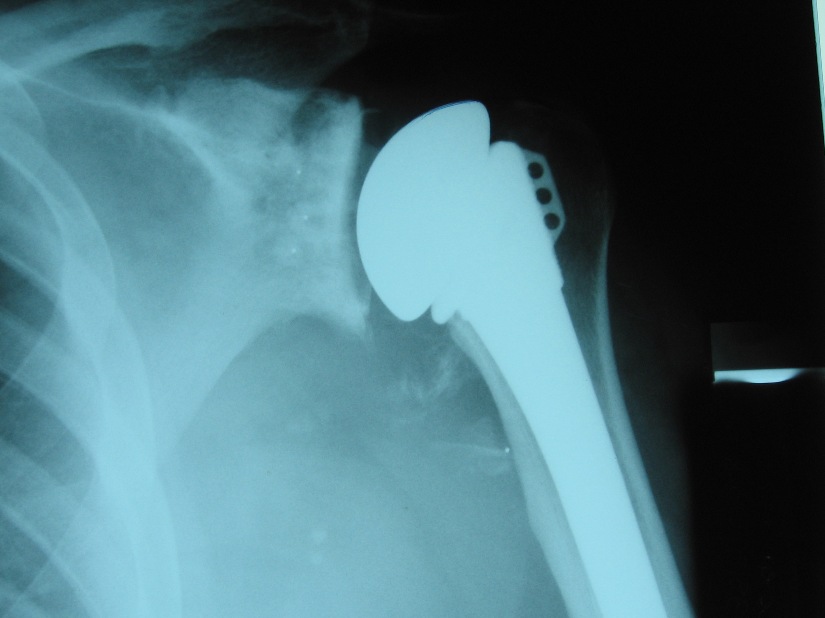
- operative considerations: hemiarthroplasty vs total shoulder arthroplasty
- anatomy:
- normal population, glenoid version: from 5 deg of anteversion to 15° of retroversion, with an
avg preop retroversion range from 1 deg to 6 deg;
- surgical goal of resurfacing is to place the glenoid in 0° of version and inclination with respect to the
plane of the scapula;
- references:
- Penetration depth and size of the nonarthritic glenoid: Implications for glenoid replacement.
- Glenoid Component Retroversion Is Associated with Osteolysis
- indications for resurfacing are controversial;
- increased glenoid loosening rates from eccentric loading & excessive wear can be expected w/ rotator cuff arthropathy;
- non concentric glenoid:
- certainly a non-concentric glenoid (ie posterior glenoid erosion) is a clear indication for glenoid resurfacing, since a congruent
joint is necessary for optimal function;
- reference:
- Recentering the Humeral Head for Glenoid Deficiency in Total Shoulder Arthroplasty.
- Posterior glenoid wear in total shoulder arthroplasty: eccentric anterior reaming is superior to posterior augment.
- component design:
- cemented peg components may be preferable to keeled components;
- hybrid concept with press fit keel and cemented pegs may be best (biomet)
- references:
- Radiographic comparison of pegged and keeled glenoid components.
- The radiographic evaluation of keeled and pegged glenoid component insertion.
- A study of micromovement of pegged and keeled glenoid components compared using radiostereometric analysis.
- Three-dimensional analysis of glenoid replacement prostheses: a comparison of keeled and pegged anchorage systems.
- Stability of cemented in-line pegged glenoid compared with keeled glenoid components in total shoulder arthroplasty.
- Radiographic comparison of pegged and keeled glenoid components using modern cementing techniques: a prospective randomized study.
- glenoid version:
- in the report by Churchill RS, et al, 344 human scapular bones (172 matched pairs) were measured for their glenoid height,
width, inclination, and version;
- overall glenoid version for the entire study group was 1.23° of retroversion;
- average glenoid version for black and white patients measured 0.20° and 2.65° of retroversion, respectively (P = .000014);
- no statistical difference in glenoid version was found between men and women of the same race;
- references:
- Glenoid size, inclination, and version: An anatomic study.
- The use of computerized tomography in the measurement of glenoid version.
- glenoid tilt:
- note that superior glenoid tilt is a risk factor for secondary rotator cuff dysfunction and eventual superior glenoid migration;
- ref: Secondary rotator cuff dysfunction following total shoulder arthroplasty for primary glenohumeral osteoarthritis: results of a multicenter study with more than five years of follow-up.
- bone loss:
- posterior bone loss:
- many w/ osteoarthritis have posterior glenoid bone loss, where as pts w/ RA may have central (medial) erosion;
- if postior glenoid erosion is present, it may be necessary to alter amount of humeral retroversion from nl 35 deg to a less
retroverted position;
- hence glenoid is positioned in more retroversion but humeral head will be in less retroversion, and therefore the 2 will
balance out;
- Outcomes of Anatomic Total Shoulder Arthroplasty with B2 Glenoids: A Systematic Review.
- bone grafting for glenoid components:
- w/ more substantial posteior erosion, then a glenoid component w/ posterior augmentation will be necessary;
- central bone loss:
- in many cases, can be managed w/ bone grafting or use of a larger portion of cement;
- reference:
- Glenoid bone-grafting in total shoulder arthroplasty.
- center point for reaming:
- center point: lateral aspect of the subscapularis fossa at a point midway between the superior and lateral borders of scapula;
- true center of glenoid is slightly inferior to midpoint - this is point of slippage of the humeral head during concentric motion;
- ref: Glenoid Perforation With Pegged Components During Total Shoulder Arthroplasty
- reaming depth:
- The subchondral bone layer and glenoid implant design are relevant for primary stability in glenoid arthroplasty
- cement mixing technique:
- The effect of cementing technique on structural fixation of pegged glenoid components in total shoulder arthroplasty.
- Complications:
- excessive offset (over stuffing the shoulder):
- "over-stuffing the shoulder" with placement of a glenoid component will lateralize the humeral component and will place the
subscapularis tendon under increased tension and risk rupture;
- avoid excessively large components and neck lengths since this will increase capsular tension and will result in decrease in
motion and increase instability;
- surgeon should be able to pass one finger between the acromion and the prosthetic head, should be able to inferiorly translate
humeral head so that one half of the glenoid is exposed;
- humeral head component should allow enough posterior translation in order to allow exposure of anterior half of glenoid (15
mm of posterior translation);
- abducted arm should allow 70 deg of internal rotation and 40 deg of external rotation;
- overstuffing the joint is more likely with total shoulder replacement (rather than hemiarthroplasty) because the glenoid
component will add to the offset;
- glenoid lossening:
- radiolucencies around the glenoid component will eventually be seen in 60% of patients;
- some authors note that in many cases radiographs may fail to show loosening because xray beam is not perpendicular to the
bone-component interface;
- flouroscopically positioned radiographs may improve radiographic diagnosis of loosening
Total shoulder arthroplasty versus hemiarthroplasty. Indications for glenoid resurfacing.
The early results of porous-coated total shoulder arthroplasty.
Survivorship of unconstrained total shoulder arthroplasty.
The Dana total shoulder arthroplasty
Total shoulder arthroplasty with the Neer prosthesis.
Indications for glenoid resurfacing in shoulder arthroplasty.