

Carl J. Basamania M.D.
- Discussion of Bankart Lesions
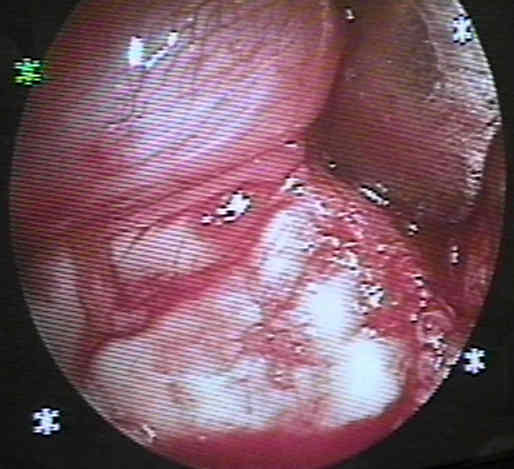
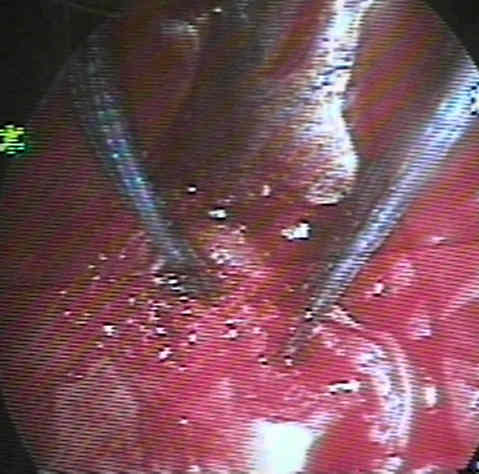
- Assessment of Bankhart Lesion:
- see: Bankhart lesion:
- a joker or similar instrument may be placed into the defect, which places the labrum under tension and allows assessment of its length;
- it is controversial as to whether labral tears less than 0.5 mm to 1 cm need to be repaired;
- if the Bankhart lesion is large enough for repair, freshen the underlying sclerotic bony surface with a rasp or burr;
- if a Bankhart lesion is not present, then consider whether the patient has a Hagel lesion (capsular avulsion from the proximal humerus);
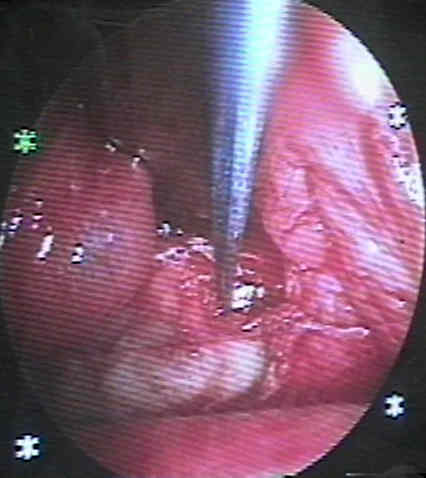
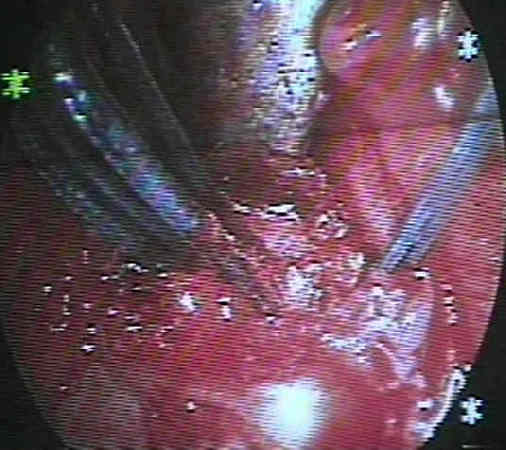
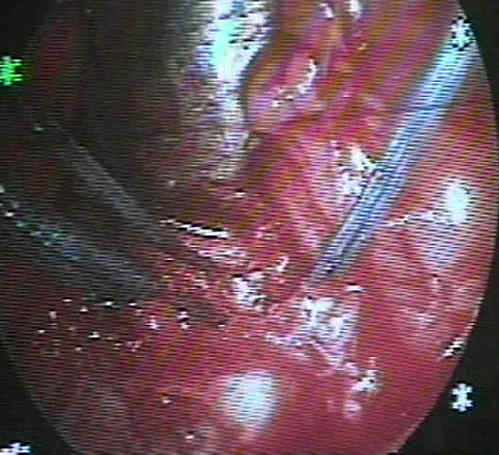
- Placement of Drill Holes:
- attempt to place anchor drill holes on the edge of the articular surface of the glenoid;
- avoid the tendency to place anchor drill holes too far medially;
- hazards:
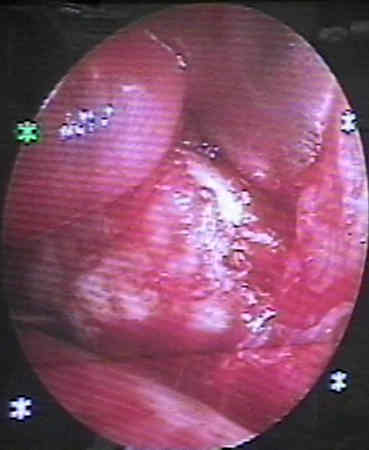



- Repaired Labrum: 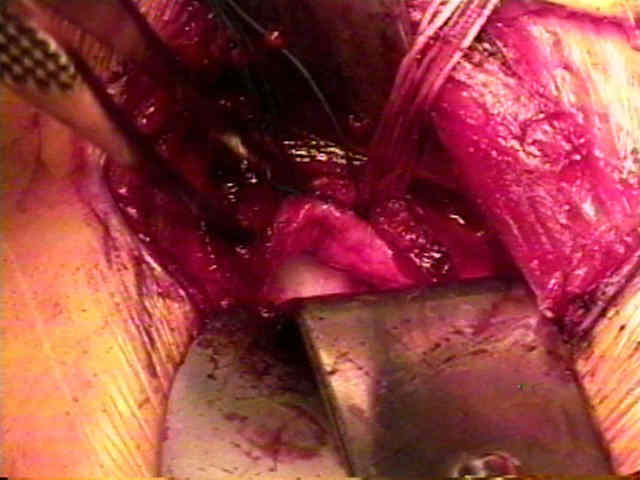
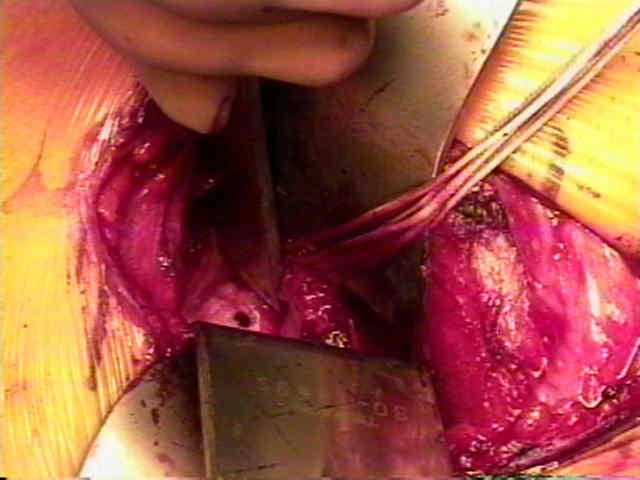
- Bankart Repair w/o Anchors:
- involves repair of defect in anterior glenoid labrum & reattaches inferior glenohumeral ligaments;
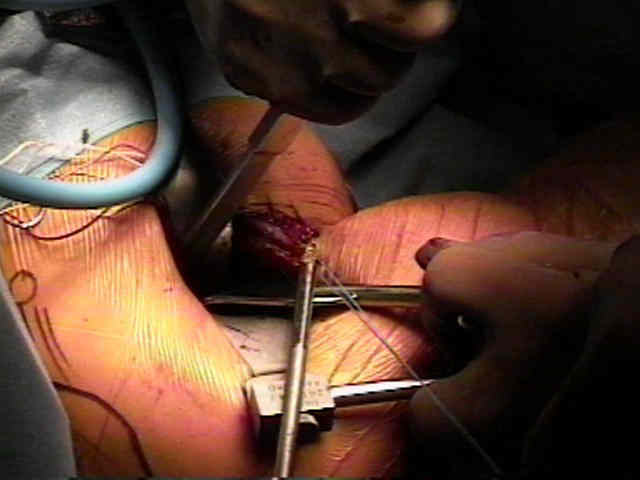
- beginning at antero-inferior margin of the glenoid, use a towel clip and awl to make approx 3 holes across the anterior 1/3 of glenoid labrum;
- through these holes are passed free needles w/ PDS suture (the middle hole needs to contain two free PDS sutures);
- the free ends of the sutures are then passed into the overlying capsule and tied down inorder to firmly oppose the capsule to the anterior margin of the glenoid;
- a capsular shift can be incorporated into the repair, by incorporating inferior capsule to the repair site
Bankart repair for anterior instability of the shoulder. Long term outcome.
The capsular imbrication procedure for recurrent anterior instability of the shoulder.
An approach to the repair of avulsion of the glenohumeral ligaments in the management of traumatic anterior glenohumeral instability.
Anterior fracture-dislocations of the shoulder: pitfalls in treatment.
Failed surgery for recurrent dislocations of the shoulder.
Failed anterior reconstruction for shoulder instability.
Recurrent anterior dislocation of the shoulder after surgical repair. Apparent causes of failure and treatment.