

- See:
- Percutaneous Pin Fixation
- Type III Supracondylar Frx
- Indications:
- vascular injuries
- inadequate reduction;
- brachialis may become interposed at frx site or by proximal humeral frx fragment button-holed thru brachialis (see physical exam);
- if this occurs, closed reduction w/ longitudinal traction may worsen tightening of the muscle around protruding fragment;
- periosteum:
- tears proximal to frx site, and may become interposed into anterior frx gap;
- w/ interposed periosteum open reduction is required;
- Surgical Approach for Inadequate Reduction:
- consider the standard posterior approach;
- alternatively limited medial and lateral incisions allow direct access to the entire surface of the fracture and should guarantee protection for the nerve;
- Surgical Approach for Vascular Injury:
- begin w/ transverse incision over antecubital fossa, and subsequently decide if further exposure is needed on the proximal-medial side vs. the distal-lateral side;
- posterolateral displacement:
- need to visualize the medial spike of the proximal fragment and to explore the median nerve and brachial artery;
- consider anteromedial approach;
- posteromedial displacement:
- need to visualize the lateral spike of the proximal fragment and radial nerve;
- consider anterolateral approach:
- w/ either approach, reduction requires hyperflexion, which precludes adequate visualization of frx site;
- attempt to palpate frx reduction as elbow is hyperflexed;
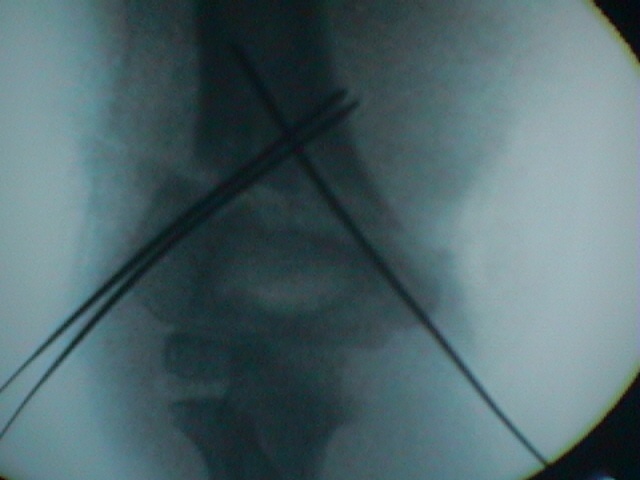
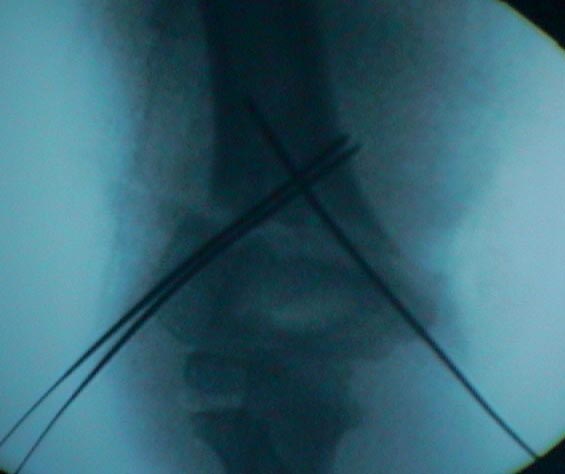
- following frx reduction, insert crossed pins thru stab incisions; (cross pinning technique);
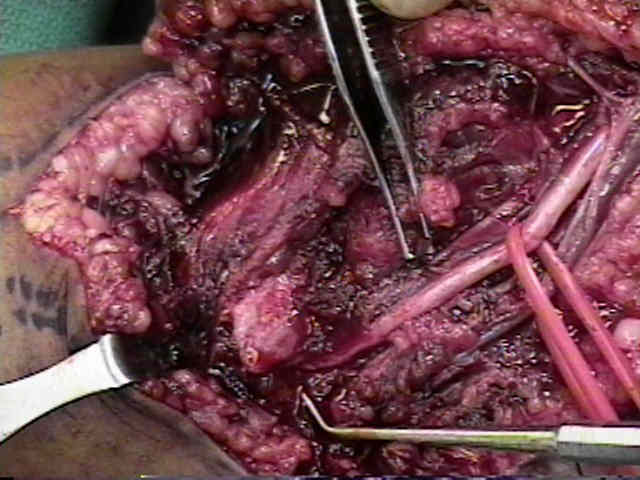
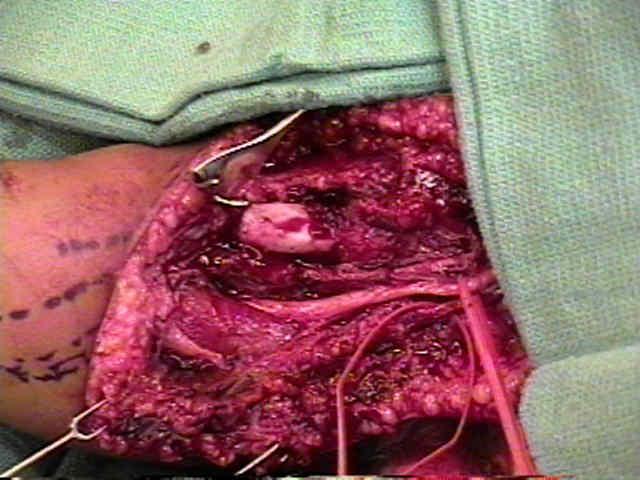
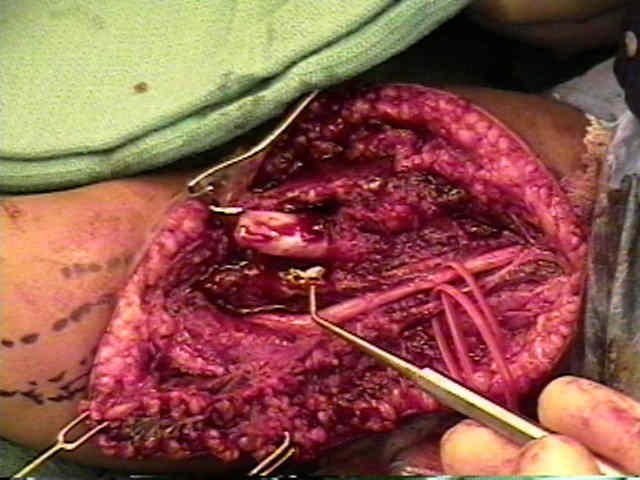
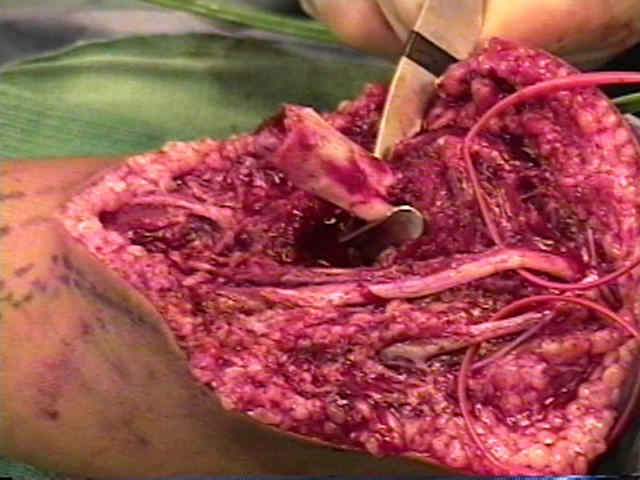
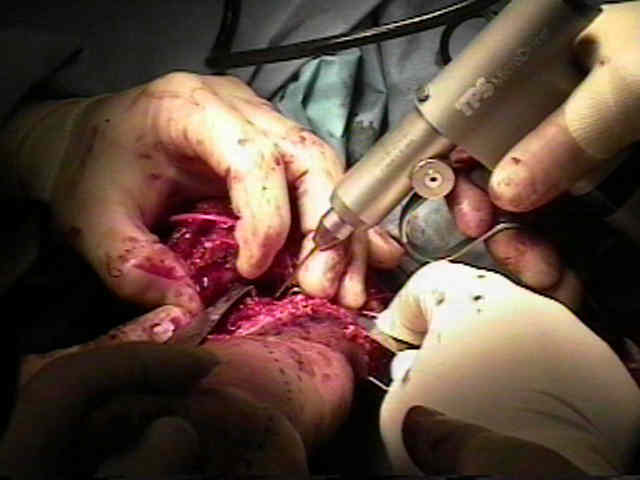
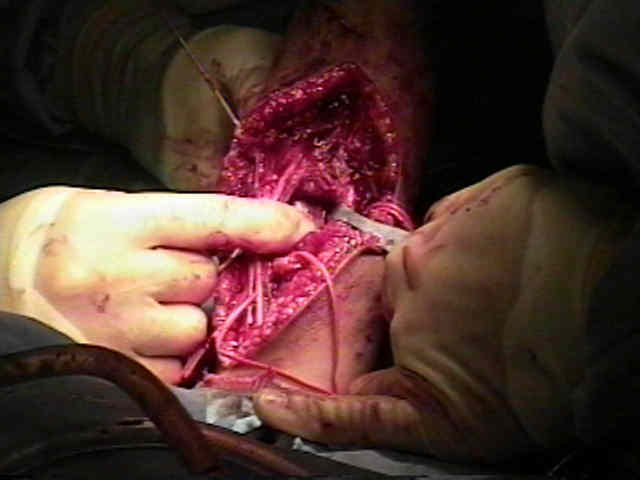
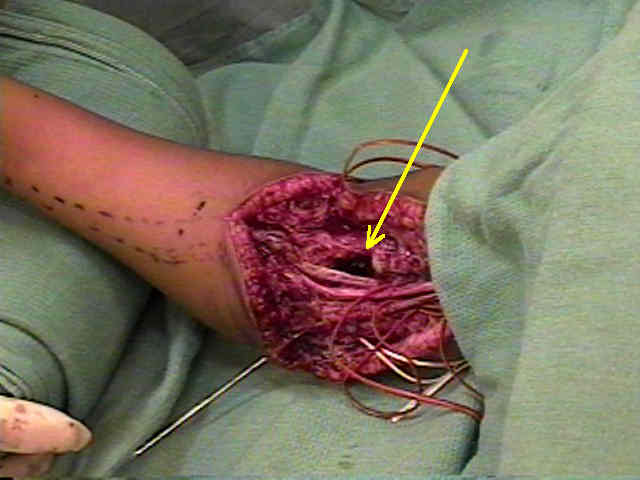
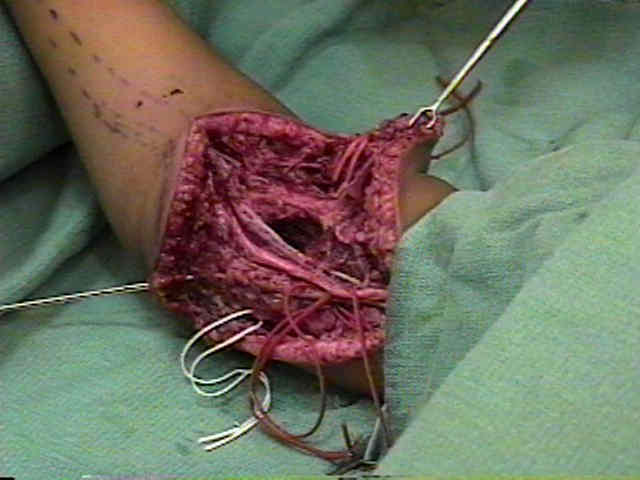
- Case Example:
- 3-year-old child who sustained a type III supracondylar fracture following a fall;
- on physical exam there was subcutaneous ecchymosis (bone has buttonholed thru brachialis);
- an attempt was made at closed reduction and pinning, but this resulted in marked decrease in pulse;
- an open reduction was subsequently performed and the brachial artery was noted to be partially entrapped at the fracture site;




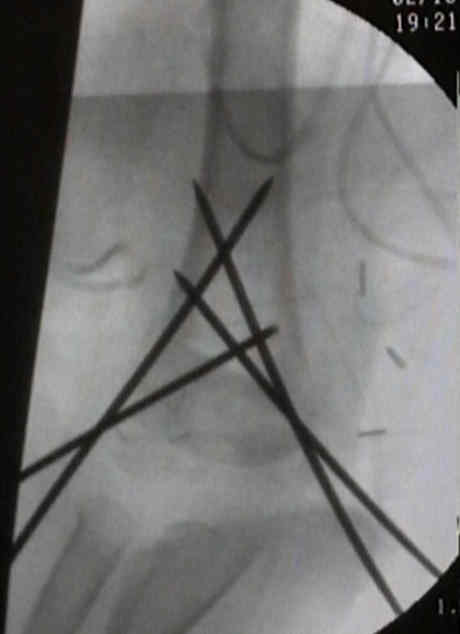
- Case Example:
- 7-year-old female who presented with a displaced supracondylar fracture - an attempt at closed reduction was carried out, but the reduction was unacceptable;
- open reduction was carried out via limited medial and lateral incisions;



Supracondylar fractures of the humerus in childhood: range of movement following the posterior approach to open reduction.
The operative management of supracondylar fractures.
The posterior approach to the elbow revisited.
The operative management of the difficult supracondylar fracture of the humerus in the child.
Operative reduction and fixation of a difficult supracondylar extension fracture of the humerus.
Open reduction and internal fixation of displaced supracondylar fractures of the humerus in children.
Supracondylar humeral fractures in children. Beware the medial spike.