


- Distal Femoral Resection
- Distal Femoral Sizing Guide (and Rotational Alignment)
- Anterior, Posterior, and Chamfer Cuts
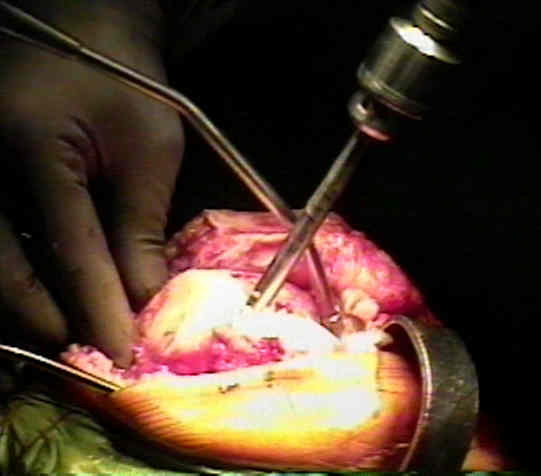
- Location of Entry Hole:
- ideally the starting point is slightly medial and posterior to the center of the notch;
- generally the drill needs to be inserted 1 cm above the notch to enter into the center of the canal;
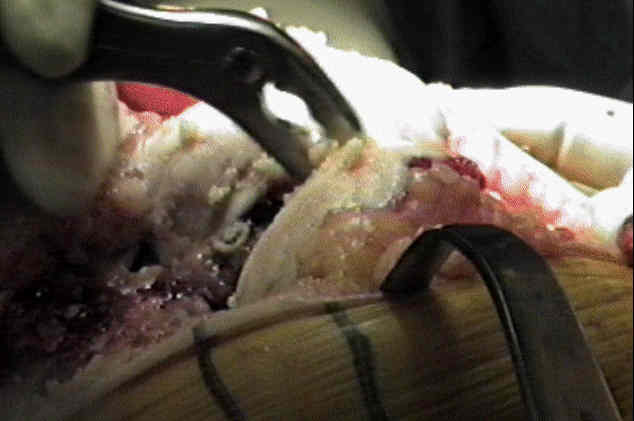
- use a rongeur to remove any residual osteophytes from the intercondylar notch;
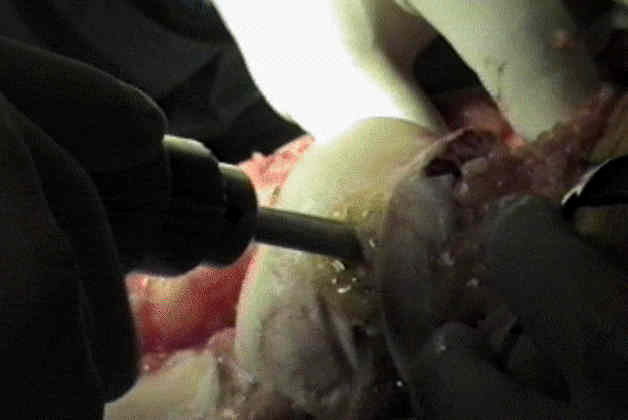
- use intercondylar drill guide to drill hole into center of medullary canal of the femur;
- use a cannulated guide rod to help prevent fat embolism
- normally the entry hole is placed slightly anterior to the insertion of the PCL (6 mm from center) on to the femur;
- excessive posterior placement most often results from mis-judging top of intercondylar notch (due to inadequate debridement
of notch osteophytes);
- placement of the drill hole too posterior can lead to flexion of the femoral component, which will complicate the subsequent
femoral cuts, and will lead to incomplete knee extension;
- generally the drill hole should be made 1 cm above the roof of the intercondylar notch, which will keep the guide rod in center
of medullary canal;
- vent the intramedullary canal by widening the drill hole in an AP direction (using a ronguer);
- this will allow the fatty contents of the medullary can to exit through the drill rather than be embolized as the alignment rod is
driven retrograde;
- to assure that medullary canal is unobstructed, pass the medullary rod into the drill hole and up the medullary canal of the femur;
- avoid pushing IM guide too far in, as the femoral bow will add some extension to the distal cutting block and may lead to
femoral notching and fracture;
- Anterior/posterior considerations: (avoid saggital cutting errors);
- medial / lateral considerations:
- rod should be inserted slightly medial to the notch center, just above the PCL insertion;
- if the rod is inserted too laterally, the distal cut will be made in excessive valgus;
- if the rod is inserted too medially, then the cut will be made in relative varus, and the distal femoral cutting guide will sit
excessively distal, (hitting the distal medial edge of the medial condyle) which will decrease the extension gap;
- if in this case, a slight medial position is dictated by the medullary antomay, then increase degree of valgus from 5 to 6-7 deg;
- ref: Intramedullary guide for femoral component positioning in TKA: How entry point affects femoral component position.
- Extra-Meduallary Guides:
- if properly applied, IM femoral alignment systems are accurate to w/in 1-2 degs of varus or valgus, & are more accurate than
extramedullary jigs;
- use of extrameduallary alignment systems may be indicated in the case of ipsilateral hip arthroplasty with a long
femoral component, mal-alignment following a femoral fracture, or in the case of excessive excessive anterior bowing;
- radiograph of the entire femur is needed, so that when the IM guide is used, allowances can be made for bowing or deformity
Effect of rotation on the axial alignment of the femur. Pitfalls in the use a of femoral intramedullary guides in total knee arthroplasty.
Extramedullary versus intramedullary alignment guides in total knee arthroplasty.
The effect of prosthetic patellar thickness and anterior femoral surface on limiting flexion in TKA. Holtgrew. Trans Orthop Res Soc.1989;14:369.
The accuracy of femoral intramedullary guides in total knee arthroplasty.
Proper entry point for femoral intramedullary guide in total knee arthroplasty.
The variability of intramedullary alignment of the femoral component during total knee arthroplasty.