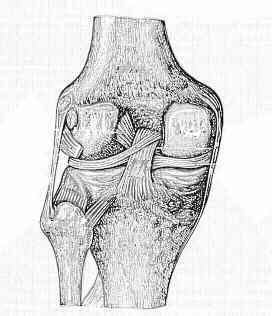
- Femoral Tunnel:
- goal is to re-create the large anterolateral band of the PCL, which tightens in flexion;
- see anatomy of PCL
- cortical entry site:
- small skin incision is made w/in Langer's lines, which overlies the vastus medialis oblique insertion into the intermuscular septum;
- usually midway between the medial femoral epicondyle and medial border of patella;
- cortical tunnel site: 2 to 3 cm from the articular surface of medial femoral condyle;
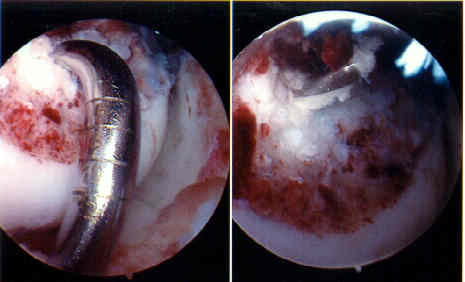
- intra-articular entry site:
- in the intercondylar notch, the guide wire is positioned about 5-15 mm posterior (or distal) to the edge of the articular surface
(anterior aspect of the notch) at the 1 to 1:30 o'clock (or 10:30 to 1
1 o'clock) position (which is 5 mm down from the top of the intercondylar notch);
- alternatively consider making the entry site about 8 mm from articular border and at the junction of medial wall and the intercondylar roof;
- in most cases, the graft will be placed on the most anterior aspect of the femoral footprint;
- as pointed out be Markolf KD, et al, excessively anteriorly placed femoral tunnels can generated excessive tension w/ flexion and should be avoided;
- moving the tunnel site anterior in the intercondylar notch results will cause the graft to excessively
lengthen in flexion and shorten in extension;
- as pointed out by Burns et al., the isometric region lies about 1 cm from the intercondylar roof in a posterior and slightly distal direction;
- sites placed distal to this site (or placed anterior as judge by the arthroscope) will lead to increases in the distance between the femoral and tibial attachment sites as the knee is flexed;
- moving the femoral tunnel in a distal-proximal direction has a much larger effect on graft tension than moving it in the AP direction;
- note that whatever graft fixation method is chosen, patients may note tenderness over the cortical fixation site if hardware is prominent;
Current Concepts Review. Injuries of the Posterior Cruciate Ligament.
The results of surgical repair of acute tears of the posterior cruciate ligament.
Bone-block transfer of the medial head of the gastrocnemius for posterior cruciate insufficiency.
Acute tears of the posterior cruciate ligament. Results of operative treatment.
Posterior tibial subluxation of the posterior cruciate-deficient knee.
Long-term followup of posterior cruciate ligament rupture: a study of 116 cases.
Arthroscopically assisted combined anterior and posterior cruciate ligament reconstruction.