


- Discussion:
- a type of cyst which results from egress of fluid through a normal communication of a bursa (semimembranosus or medial
gastrocnemius bursa) or may be caused by herniation of the synovial membrane through the joint capsule;
- symptoms develope most often in bursa beneath the medial head of gastrocnemius or in the semimembranous bursa;
- later is a double bursa located between the semimembranosus tendon and the medial head of the gastrocnemius;
- Baker's cysts are usually located at or below the joint line, whereas cysts of semimembranous bursa are above the joint line;
- diff dx: popliteal mass:
- children:
- popliteal cysts (Baker's cysts) are common in children, occurring more often in boys & usually found in medial aspect of popliteal fossa.
- in children popliteal cyst infrequently communicates w/ joint and intraarticular pathology is rare;
- however, consider lipomas, xanthomas, vascular tumors, fibrosarcomas;
- (the popliteal cyst should transilluminate)
- if dx is in doubt, ultra-sound can distinguish between fluid-filled cyst and a solid tumor;
- radiographs should be studied for soft tissue calcification in the mass, which may indicated synovial cell sarcoma or hemangioma;
- in children, surgical excision of popliteal cysts is rarely indicated.
- most authors report spontaneous resolution of cysts in 10-20 months;
- therefore, a prolonged period of observation is strongly recommended before surgical excision is considered.
- in protracted cases, cysts may respond to aspiration and steroid injection, (note that unlike adults, the cyst may not be intra-articular, and therefore,
may respond to aspiration);
- references
- Popliteal cysts in children. The case against surgery.
- Baker's cyst in children: Is surgery necessary?
- adults:
- in adults, intra-articular pathology is common, & cyst may recur if intra-articular pathology is not corrected;
- cysts are connected to the knee joint through valvular opening;
- presence of knee effusion (excessive fluid pressure), allows unidirectional egress of fluid through the valve and into the cyst;
- cyst is locacted between the semimembranosus tendon and the medial head of gastrocnemius tendon;
- if cyst lies in atypical location consider tumor (see diff dx);
- reoccurrence of the cyst is common following surgical removal, and therefore treatment is directed toward intra-articular pathology;
- meniscal tears:
- some popliteal cysts are caused by a lesion of the posterior third of the medial meniscus;
- posterior horn meniscal tears which extend to capsule may cause a defect (1 way valve) to develop between joint cavity and gastro-semimembranosus bursa;
- cyst is usually located posteromedially & as it enlarges, it dissects plane between the gastrocnemius and underlying soleus.
- partial meniscectomy for tears will usually to resolution of cyst;
- in the report by Sansone V and De Ponti A, the authors treated 30 patients w/ Baker's cyst w/ mean followup of 32 months;
- arthroscopy demonstrated a connection between joint space and cyst in all patients;
- surgical goal involved removal of anatomic structures imposing the one-way passage of fluid from the joint space into the cyst;
- in 27 of 30 cases, there appeared an oval opening located between the body and the posterior horn that extended to the articular capsule;
- a blunt instrument could be easily introduced into the opening, and just a slight amount of pressure was needed to overcome the capsular plane;
- attempt to feel the point of the instrument under the skin, to the posteromedial site;
- all of the structures which obstructed the capsular orifice were removed (fibrous septa, bands, meniscus flaps);
- a motorized shaver is used to created a capsular opening of about 4 to 5 mm in diameter;
- 2 years after the treatment, good clinical results were seen in 95% of patients;
- ref: Arthroscopic treatment of popliteal cyst and associated intra-articular knee disorders in adults.
- in absence of meniscal pathology, removal of cyst, closure of communication w/ joint, and suture of the medial head of gastrocnemius to
posterior capsule can be performed in symptomatic individuals;
- chondral injury:
- in the report by S. Rupp et al 2002, the authors prospective studied the prevalence of popliteal cysts and the associated intraarticular
lesions in a group of 100 patients wheo underwent knee arthrscopy;
- prevalence of popliteal cysts was 20% in the study group and 0% in the control group;
- patients with a popliteal cyst had a significantly higher prevalence of medial meniscal tears (70% versus 19%) and of chondral lesions (85% versus 28%);
- tears of the lateral meniscus, however, were more evenly distributed (20% versus 36%);
- 16 of 20 patients with a popliteal cyst were available for a follow-up examination 1 to 3 years after the arthroscopic procedure.
- 11 popliteal cysts had persisted and chondral lesions were the most relevant prognostic factor;
- the authors concluded that the popliteal cyst was a secondary phenomenon and that treatment should address the underlying intraarticular lesions;
- ref: Popliteal Cysts in Adults. Prevalence, Associated Intraarticular Lesions, and Results after Arthroscopic Treatment
- giant synovial cysts of calf have been reported in pts w/ RA (long-standing RA synovitis of knee can cause popliteal cyst formation);
- rupture of the cyst results in dissection of synovial fluid distally into calf & can present in a manner similar to thrombophlebitis;
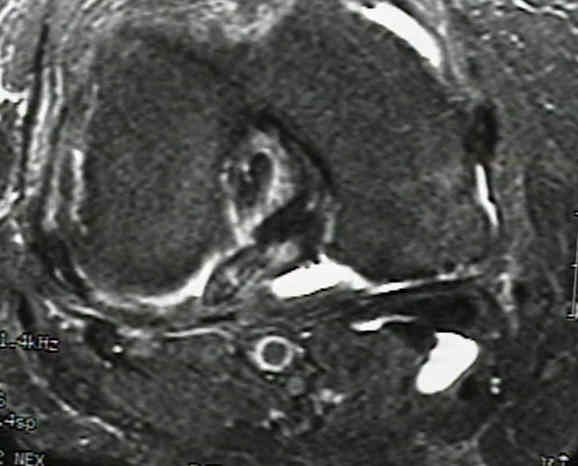
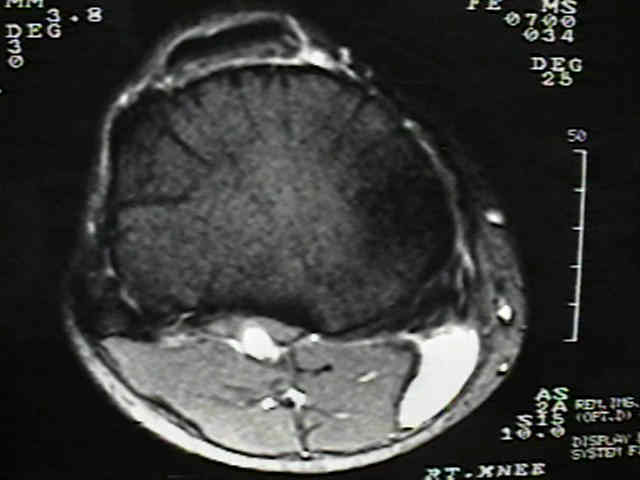
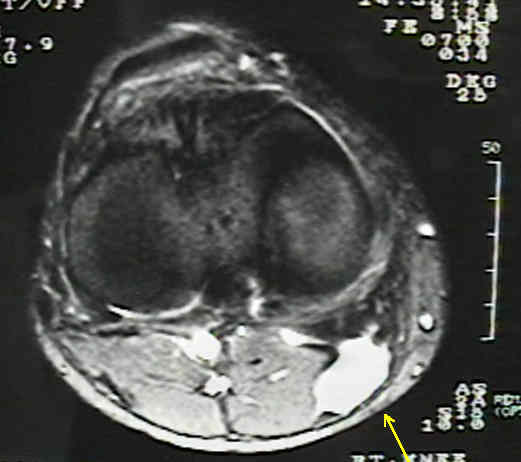
- MRI Findings:
- fluid filled mass produces an intermediate signal on T1 proton density weighted image and high signal on T2 images;
- cyst should always lie medial to the lateral head of the gastrocnemius muscle

On the formation of synovial cysts in the leg in connection with disease in the knee joint. 1877.
Ruptured Baker's cyst causes ecchymosis of the foot. A differential clinical sign.
Proximal dissection of a popliteal cyst with sciatic nerve compression.
Arthroscopic treatment of popliteal cyst and associated intra-articular knee disorders in adults.
Popliteal Cysts: A Current Review