

Hip Arthroscopy
(see also hip joint and hip capsule)
Indications
- evaluation of hip pain - candidates are patients with nonspecific radiographic findings and reproducible, functionally-limiting
exam findings;- false negative rate of plain x-ray, bone scan, CT, arthrogram, and routine MRI has been quoted as high as 80% in some
patient populations. - gadolinium enhanced MRI demonstrated a sensitivity of 55% for all intra-articular pathology and 74% for labral tears in
patients where other modalities had failed to reveal a source of pain' - reference: McCarthy, Current Concepts in Joint Replacement, 1997.
- false negative rate of plain x-ray, bone scan, CT, arthrogram, and routine MRI has been quoted as high as 80% in some
- synovitis - diagnosis and biopsy can be performed with arthroscopy.
- limited synovectomy can be performed (total synovectomy currently requires open procedure with head dislocation);
- loose bodies - post-traumatic OCD fragments and loose bodies associated with OCD and synovial chondromatosis, bullet
fragments, and cement fragments (s/p dislocated THA that was reduced closed) have been reported. - labral tears- an increasingly common entity following hip trauma resulting in persistent pain.
- tears are more common in individuals with acetabular dysplasia.
- in study by McCarthy, et al (1998), 18/20 patients w/ symptomatic dysplasia had labral tears, and 85% of these improved w/ arthroscopic debridement;
- authors recommend avoidance of over resection of the degenerative labrum;
- debridement brings excellent relief unless there are associated degenerative changes, acetabular dysplasia, or acetabular
chondral defects > 1cm. - septic arthritis - (Blitzer): small series where infections were treated with arthroscopy, drain placement through cannulae, and antibiotics.
- osteoarthritis - role currently unclear; - may be helpful in staging or planning for osteotomies. minimal lavage benefit.
Contraindications
- conditions that limit exposure and benefit (e.g., acetabular protrusio, advanced arthritis)
- Hip arthroscopy for acetabular dysplasia: a pipe dream?
Anesthesia and Positioning
- GETA, LMA, or spinal anaesthesia
- fracture table is utilized for traction;
- note that the leg should be slightly abducted to allow for efficient hip distraction;
- be aware that excessive traction has been associated w/ sciatic nerve palsy;
- supine (our preference) or lateral on a fracture table - coban wrap is used on the foot to control rotation / 0 degrees ER, flexion,
and abduction. - minimal distraction initially;
Anterolateral Portal
- HipHip arthroscopy: an anatomic study of portal placement and relationship to the extra-articular structures.
Lateral Portal
- lateral portal is typically utilized for the arthroscope and the anterolateral portal is used for instrumentation;
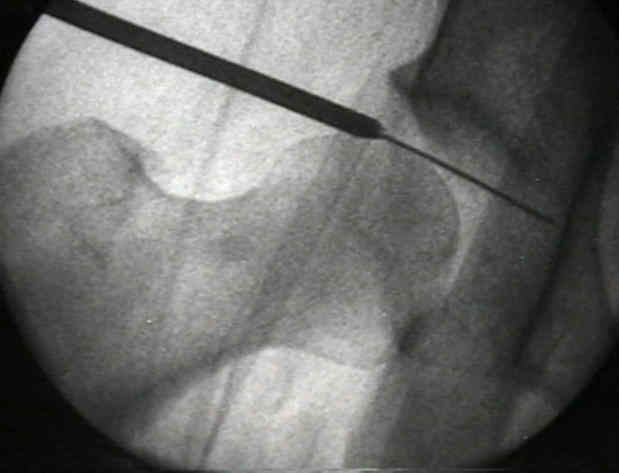
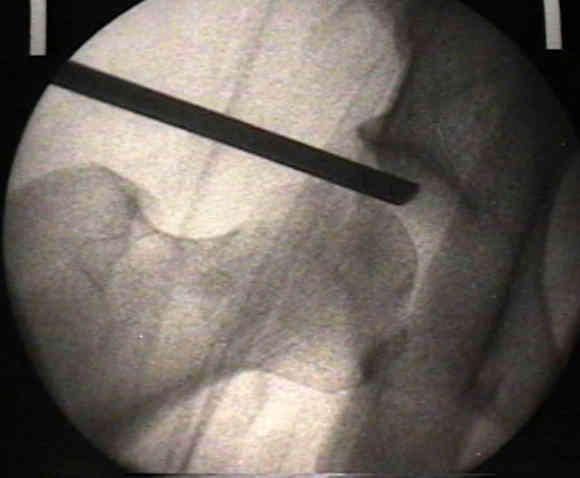
- 14 gauge angiocath 2 cm over anterior 1/3 greater troch and parallel to floor under fluoro showing an AP
of the hip;- aim just below labrum toward the sourcil (wt-bearing portion of acetabulum)
- 14 gauge angiocath is inserted first and saline is injected in order to relieve intra-articular vaccum;
- air arthrogram will often be noted on flouro upon entering the joint.
- inject 50cc NS and increase distraction since negative joint pressure released;
- remove 14 gauge needle and place guide rod through angiocath.
- a Nitenol guide wire can then be passed thru the angiocath and into the joint;
- blunt dilator through soft tissues to joint capsule using fluoroscopy.
- sharp dilator through capsule using fluoroscopy (gentle)
- larger blunt dilator through capsule into joint
- remove dilator and place cannulated 30 degree scope (70 degree scope can also be used)
- optics are often blurry at this point







Anterior Portal
- the lateral portal is typically utilized for the arthroscope and the anterolateral portal is used for instrumentation.
- insertion point lies at the intersection of the ASIS (verticle line) and the symphysis (horizontal line), which should place it lateral
to the femoral nerve and several finger breadths below the femoral head;- some surgeons insert the cannula thru the skin 1-2 cm below the tip of the greater trochaner;
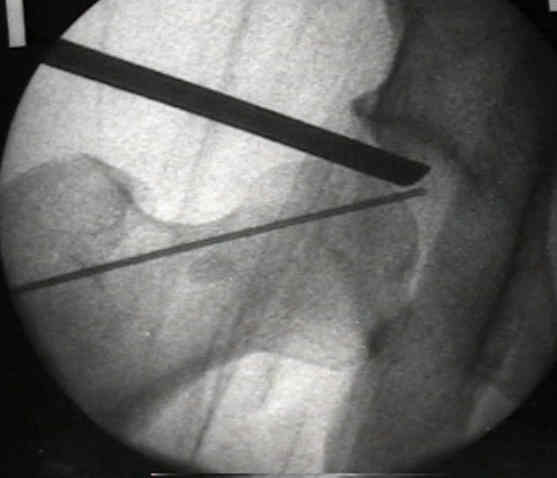
- use the 14 gauge angiocath to create an anterolateral portal.
- angiocath is advanced along the femoral neck 45 degrees medial, 45 degrees proximal, and 45 degrees posterior to the skin
entry point. - saline will flow out of the angiocath upon joint entry.
- angiocath is advanced along the femoral neck 45 degrees medial, 45 degrees proximal, and 45 degrees posterior to the skin
- this portal should be dilated and the joint entered as previously described for the lateral portal.
- direct visualization should be utilized to decrease the incidence of chondral damage.
- optics should improve with outflow through this new portal.
- hazards: lateral femoral cutaneous nerve can be damaged through this approach;
Limited Anterior Exposure
- limited anterior exposure may facilitate technical difficulties of hip arthroscopy;
- modified 4-cm Smith-Petersen anterior approach to the hip exposing the joint capsule as manual traction is applied;
- 4-cm bikini skin incision is made anteriorly in the line of the skin crease 1 cm below the level of the AIIL;
- arthroscope is then easily introduced making visualization of the hip joint possible;
- internervous plane between the tensor fascia latae and the sartorius is dissected bluntly;
Arthroscopic Removal of Loose Hip Joint Fragments
(see also hip dislocations)
- avoids the need for the standard posterior or anterior approach;
Cautions
- in report by Bartlet CS, et al (1998), a cardiac arrest occurred as a result of fluid extravasation into abdomen during
hip arthroscopy (performed to remove intra-articular loose bodies from acetabular frx); - reference: Cardiac arrest as a result of intraabdominal extravasation of fluid during arthroscopic removal of a loose body from the hip joint of a patient with an acetabular fracture.

 -
-

Complications
- injury to the lateral femoral cutaneous n. can be temporary or permanent with anterolateral portal placement.
- neuropraxia of the pudendal or sciatic nerves are usually due to excessive traction and resolve with time.
- sciatic nerve can be permanently injured with posterolateral portal placement especially if extremity is externally rotated
during portal placement.- a mini-open portal is always recommended when posterolateral exposure is needed.
- sciatic nerve palsy is more likely to occur in conditions such as traumatic dislocation of the hip (loss of ligamentous
constraints);- if arthroscopy is indicated in order to retrieve an intra-articular frx fragment, be sure to avoid over distraction of the hip;
- sciatic nerve can be permanently injured with posterolateral portal placement especially if extremity is externally rotated
- pressure necrosis of the foot or perineum due to excessive force and duration of traction.
- chondral injury - common
- infection - rare
- broken instruments
- systemic complications (e.g., PE) rare
Misc
- generally can use standard knee arthroscopy equipment except in obese individuals.
- rarely find it necessary to create the more dangerous posterior portals.
References
- Arthroscopy of the hip.
- Arthroscopic anatomy of the hip.
- The acetabular rim syndrome. A clinical presentation of dysplasia of the hip.
- Hip Arthroscopy: Management problems. Hip arthroscopy for acetabular dysplasia. A Pipe Dream?
- The role of hip arthroscopy in the elite athlete.
- Hip arthroscopy: surgical approach, positioning, and distraction.
- A Catastrophic Complication of Hip Arthroscopy