

- See: Lateral Approach
- Discussion:
- allows exposure of the entire distal humerus as well as radial head, radial neck, and biceps tuberosity;
- indications for this approach include frxs of distal humerus, old posterior elbow dislocations, radial head frx, radial head excisions, arthroplasties, fixation of distal biceps tendon rupture, and resection of proximal radial-ulnar synostosis;
- it is also indicated for elbow flexion contractures
- approach is anterior to ligaments that stabilize the ulna to humerus, which decreases the chance that they could be inadvertently injured;
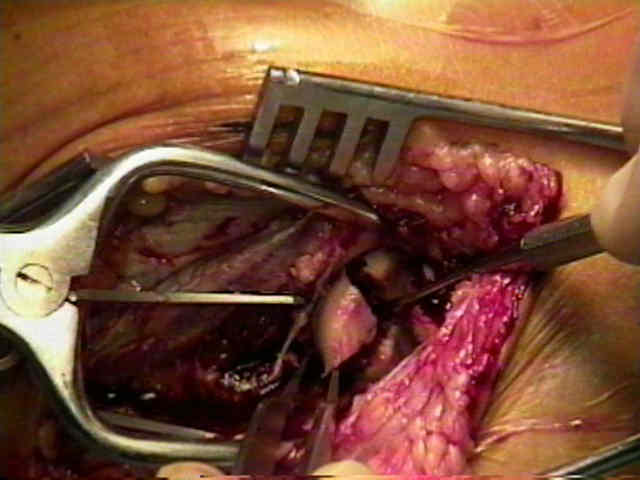
- interneural interval: (Kocher's interval);
- between the anconeus and the ECU;
- some consider the Kocher Approach to be safer than the lateral approach, since it affords protection to the PIN by going between
the anconeus and the ECU;
- in contrast, the lateral approach, which may injure the PIN by going thru the EDC and ECRL interval;
- Position:
- semilateral position:
- bump placed under the scapula, and arm draped over chest;
- be sure that positioning allows for good flourscopic visualization;
- supine position:
- main disadvantage is that visualization can be difficult;
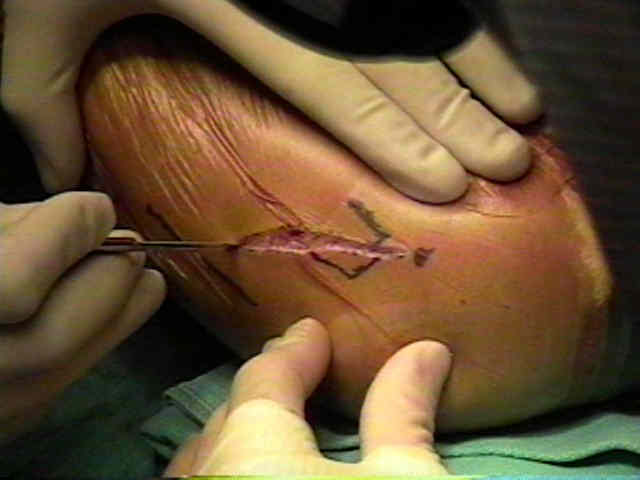
- Incision:
- begin skin incision over the lateral epicondyle (or proximal to it) & continue it distally and obliquely directly over lateral epicondyle to end at proximal ulna;
- incise through the fascia overlying the anconeus and the ECU;
- keep this dissection in line with the fibers of the ECU (not the axis of the arm) inorder to preserve the fascial contributions of the ECU to the posterolateral ligamentous
complex (see posterolateral instability);
- realize that the fibers of the anconeus are fan shaped (horizontal-proximally and vertical distally);
- keep the arm pronated during this dissection in order to avoid injury to the PIN;

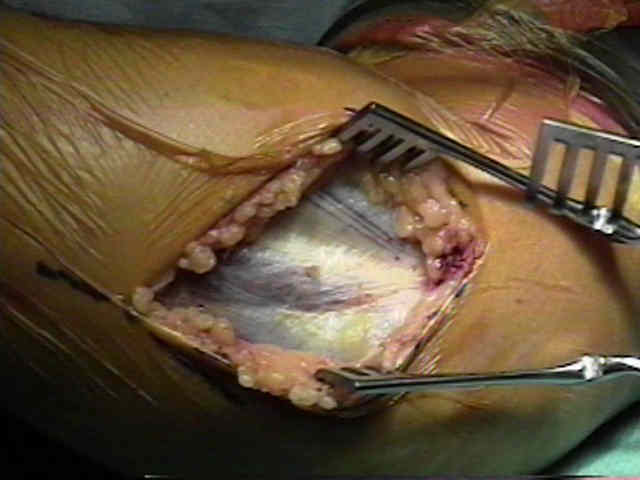
- bluntly dissect through this interval and dissect down to the joint capsule;
- the interval between these muscles is more easily found distally, since these muscles share a common proximal fascial origin;
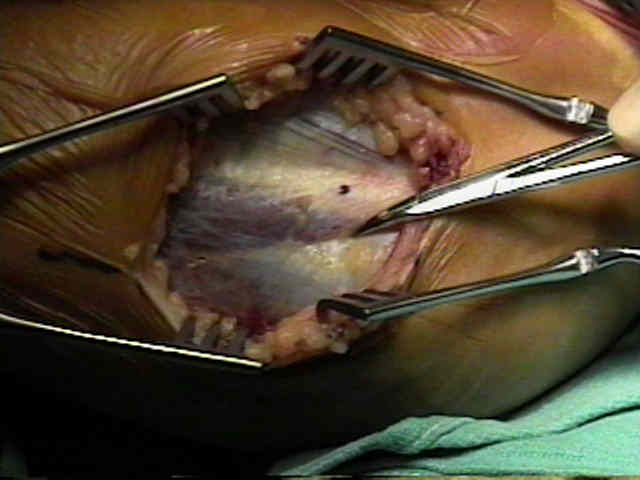
- ECU and a portion of supinator are elevated off capsule and are elevated anteriorly;
- PIN is protected at this point by the ECU and EDC
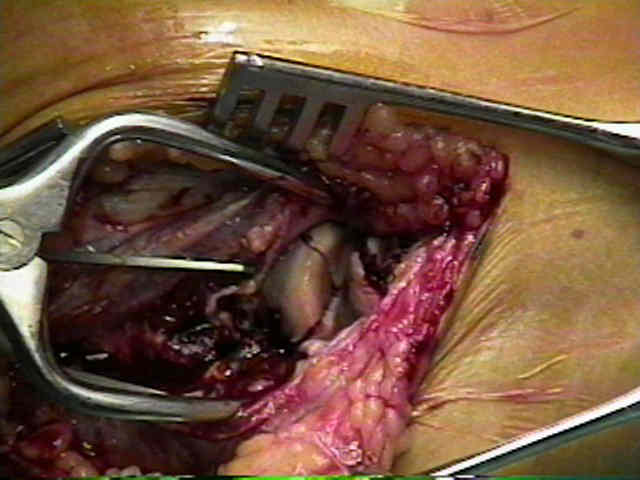
- sub-periosteally dissect the aconeus off its humeral origin inorder to expose joint capsule;
- posterior retraction, exposes the crista supinatoris;
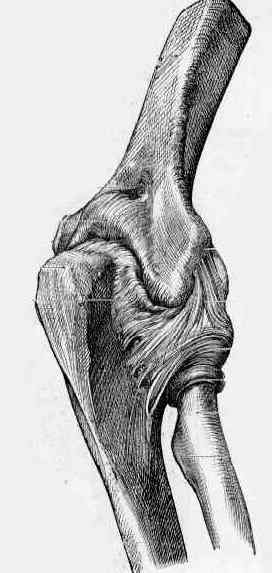
- LCL complex:
- at this point the LCL should be exposed;
- visualization of the LCL, is achieved thru anterior retraction of EDC and ECU;
- it is essential to avoid damage to the LCL complex;
- capsular incision should be made anterior to radial humeral ligamentous complex;
- incision over the radial head in line w/ the radius should avoid the LCL (avoids posterolateral instability);
- exposure of the radial head:
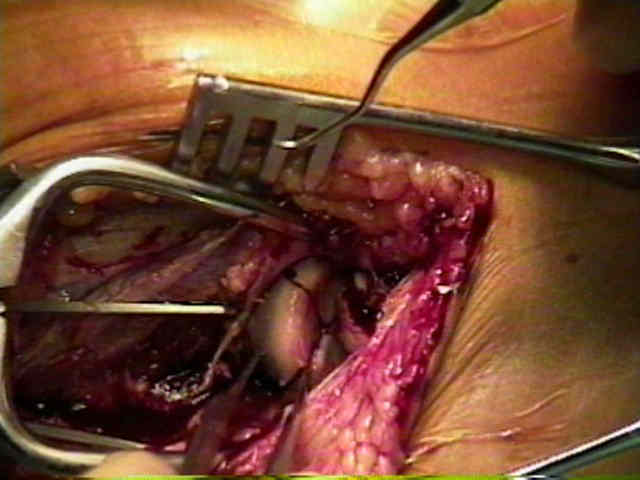
- extened exposure w/ release of LCL:
- w/ LCL clearly identified, sharply release the LCL off of the lateral epicondyle;
- this allows the elbow to be "booked open" which affords excellent exposure;
- the LCL is re-attached to the lateral epicondyle through 2 drill holes, using non-absorbable suture;
- distal exposure:
- exposure distal to the annular ligament risks damage to the PIN;
- if annular ligament must be incised consider "z" step cut for later repair;
- extended proximal exposure:
- proximally define the interval between the triceps and ECRL / BR;
- the triceps is retracted posteriorly and the BR retracted anteriorly;
- posterior border of common extensors is defined and is retracted anteriorly;
- it is important to keep line of dissection inferior to the epicondyle in order to avoid posterolateral ligamentous structures which lie anteriorly;
- EDC and anconeus can be elevated off ulna, and retracted proximally and anteriorly;
- after the common extensors have been elevated anteriorly, posterior border of the supinator is identified;
- posterior fibers of the supinator are then released off the ulna, and is reflected anteriorly, w/ care not to injure the radial nerve;
- alternatively the supinator should be released off of the ulnar border of the radius;
- pronation of the forearm will help protect the nerve during the dissection;
- wound closure:
- aconeus is sutured back into anatomic position;
- Hazards:
- PIN may be injured as it passes w/ in substance of supinator at level of radial tuberosity & continues to wind around shaft of radius
as it passes distally to the dorsum of forearm;
- avoid injury to nerve, by not extending incision distally & avoid dissection beyond radial neck;
- at the distal end of the wound, the first PIN branches at risk are those to the ECU, which are 6 cm from the radial head;
- hence it is safe to expose the proximal radius as far as the bicipital tuberosity;
- note: 1 cm of nerve translation can occur w/ forearm pronation and supination;
- pronation will position PIN farthest away from surgical field;
- capsular incision is not placed too poster or directed too obliquely because of risk of injury of posterior fibers of LCL complex;
- fibers are called lateral ulnar collateral ligament, & their disruption may result in late instability of the elbow;
- Kocher interval, in which capsular incision is made anterior to inferior aspect of radial humeral capsular ligamentous complex
- ref: The course of the posterior interosseous nerve in relation to the proximal radius: is there a reliable landmark?
The lateral approach for operative release of post-traumatic contracture of the elbow.
The posterior interosseous nerve and the posterolateral approach to the proximal radius.