

Discussion
- trimalleolar fractures involve frx of the medial and lateral malleoli along w/ a frx of the posterior lip of tibial plafond;
- frx fragment results from avulsion by the posterior tibiofibular ligament at its site of attachment to the tibia;
- clinical results triamalleolar frxs are generally worse w/ larger fragments involving a larger portion of the tibial plafond;
- irregularity in the tibial articular surface of tibia is brought against wt bearing surface of talus, & w/motion & wt bearing severe DJD develops;
- associated injuries:
Indications for Surgery
- > 25% of posterior articular surface is involved;
- fragment must have a tibial articular surface that is large enough to provide a stable wt bearing surface;
- fracture is displaced more than 2 mm;
- ankle fracture dislocation w/ posterior malleolar fracture;
- posterior subluxation of talus;
- even slightlest posterior subluxation of talus on articular surface of tibia is not acceptable;
- if frx prevents reduction of fibula;
- valgus tilt of talus in postreduction film may be a relative indication;
- syndesmosis fracture:
- - congruity of the syndesmosis is more accurately restored when a posterior malleolar fracture is fixed as compared with syndesmotic reduction alone;
Radiographs
- lateral x-ray may underestimate size of fragment because fracture plane is usually oblique to this view;
- oblique films or occassionally CT may be useful;
- "isolated posterior malleolar frx":
- note that an apparent isolated posterior malleolar frx may occur along with a Maisonneuve fracture;
Non Operative Treatment
Surgical Treatment
- generally, it is wise to approach any trimalleolar frx thru a posterior approach, if there is any chance that posterior fragment will require fixation;
- fibula fracture is reduced and fixed, thru a posterior approach using antiglide plate;
- then thru posterior approach, bluntly dissect between peroneal tendons and FHL to reach the posterior surface of tibia;
- usually the posterior fracture is located more laterally;
- adequacy of reduction is determined by palpation of extra articular frx line (intra-articular frx cannot be visualized because talus blocks joint visualization);
- in some frxs this may not be reliable due to comminution along edges of avulsed tubercle;
- in most cases, anatomic reduction of lateral malleolar frx will reduce the posterior malleolar fragment because of firm attachment of posterior tibiofibular ligament;
- this decreases tibiotalar instability, even in absence of direct fixation of posterior malleolar fragment;
- dorsiflexion of the foot may assist in reduction by a ligamentoaxis effect from the posterior capsule and posterior tibiofibular ligament;
difficulty w/ reduction
- may result from poor visualization of the articular surface;
- ligamentous attachment of fracture fragment to fibula by posterior tibiofibular ligamenty may make manipulation difficult;
- reduction is facilitated by using a large reduction clamp (pelvic reduction clamp), w/ one end inserted onto anteromedial portion of distal tibia, and other end inserted through the posterior incision directly onto the frx fragment;
- a twisting motion of wrist is used to bring frx fragment out to length and to achieve reduction of the extra-articular frx line;
- provisional stabilization w/ K wires & x-ray confirmation of reduction is obtained before screw placment;
Frx Fixation
- frx is fixed w/ 1-2 cancellous screws placed from posterior to anterior;
- use partially threaded 4.0 mm cancellous lag screws for fixation;
- care is taken to aim screw proximally enough to avoid the convex joint surface;
author's preferred technique:
- guide wires are inserted from anterior to posterior;
- - once the guide wire reaches the posterior malleolus, the wire length is measured;
- - guide wire is then driven more posteriorly, and the surgeon's gloved finger palpates the tip of the guide wire, and ensures that guide wire has properly engage the center of the posterior malleolar fragment;
- guide wire is then driven posteriorly, until it exits the posterior skin;
- cannulated screw is then inserted from posterior to anterior;
alternative fixation
- screws are placed from anterior to posterior;
- lag screws are placed thru a separate anterior incision;
- cortical screw can by placed as lag screw, or 4.0 mm cancellous screw;
- if cancellous screws are used, a short thread is required;
problems include
- frx may displace during passage of drill bit or screw;
- may be difficult to achieve lag screw effect (no screw threads w/ purchase on both sides of frx) in small posterior fragment;
Post Op
- wt bearing must be delayed until union is solid, and this may require 3-4 months for solid union;
- AVN of the posterior tibial margin can be a problem;
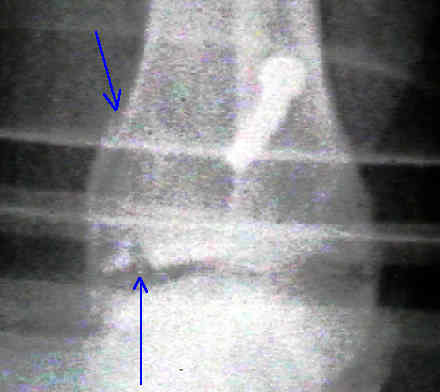
Case Example
- 30 yo female who sustained an ankle frx dislocation w/ a posterior malleolar frx;
- preoperatively the posterior malleolar fragment appeared quite large, and plans were made for fixation with cannulated screws;
- following reduction of the lateral malleolus, however, it was apparent that the posterior malleolus had self reduced, was stable, and was significantly smaller than had been thought (no fixation was needed);





- Effect of Posterior Malleolus Fracture on Syndesmotic Reduction
- Posterior malleolus fractures worth fixing
- The Joint-Contact Area of the Ankle. The Contribution of the Posterior Malleolus.
- Posterior malleolar fractures of the ankle associated with external rotation-abduction injuries. Results with and without internal fixation.
- Assessment of the posterior malleolus as a restraint to posterior subluxation of the ankle.
- Tibiotalar contact area. Contribution of posterior malleolus and deltoid ligament.
- Posterior Malleolar Stabilization of Syndesmotic Injuries is Equivalent to Screw Fixation
- The posterolateral approach to the tibia for displaced posterior malleolar injuries
- Pathoanatomy of posterior malleolar fractures of the ankle