- Tibial Tunnel:
- saftey measures:
- surgeons who do not perform this operation frequently should use flouroscopy for this tunnel;
- apply Jacobs chuck for a preset distance on the guidewire to make it less likely for the wire to pass beyond posterior cortex (and injury NV structures);
- consider making an extracapsular posterior medial incision which will allow surgeon's finger to be positioned between posterior capsule and N/V structures;
- usually, the tibial tunnel will be anchored first, the graft pretensioned, and then the femoral tunnel will be achored;
- cortical entry site:
- incision: 5 cm longitudinal incision made below and medial to tibial tubercle;
- some authors make this tunnel distal and medial to the ACL tibial tunnel site (approx 2 cm distal) when ACL reconstruction is required;
- other surgeons, will place the tunnel lateral to the tibial tubercle when ACL reconstruction is required;
- tunnel should begin well below tibial tubercle and is directed posteriorly so that it penetrates the posterior cortical surface 5-10 mm below joint line;
- a steep incline may risk blowing out the posterior tibial wall;

- articular entry site:
- prior to drilling the tibial tunnel, the tibial insertion of the posterior capsule should be freed with a curette (use
postero-medial portal or the central portal);
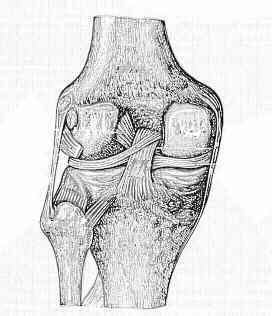
- tunnel should lie in center of PCL insertion, just lateral to midline in a depression between two tibial plateau surfaces (distal to level
of the articular surface at the distal portion of the posterior tibial edge);
- note that the posterior cruciate ligament attaches 1-2 cm below the joint line;
- hence avoid the tendency to place the tunnel too close to the surface of the tibial plateau;
- for the ligament to function properly the tunnel must not exit too anteriorly;
- hazards: popliteal artery injury:
- increasing knee flexion reduces, but does not completely eliminate, the risk of arterial injury during arthroscopic PCL reconstruction;
- maximum mean distances were noted at 100° of flexion in both the axial (9.9 mm) and sagittal (9.3 mm) planes;
- Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle. Implications for posterior cruciate ligament reconstruction.
- it is important to smooth out the sharp edges of the tibial tunnel to facilitate graft passage and to prevent fraying of the graft fibers;
- cautions:
- if a concomitant ACL reconstruction is required
- reference:
A simplified approach to the tibial attachment of the posterior cruciate ligament.
Reducing the "killer turn" in posterior cruciate ligament reconstruction by fixation level and smoothing the tibial aperture.