

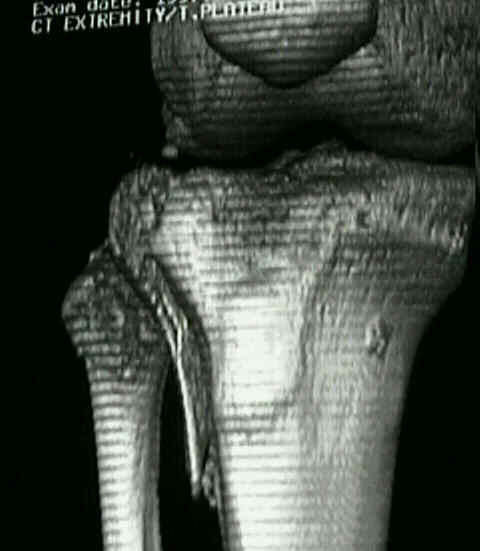
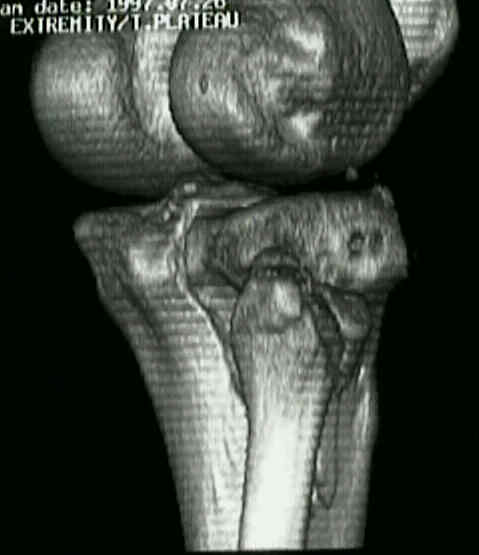
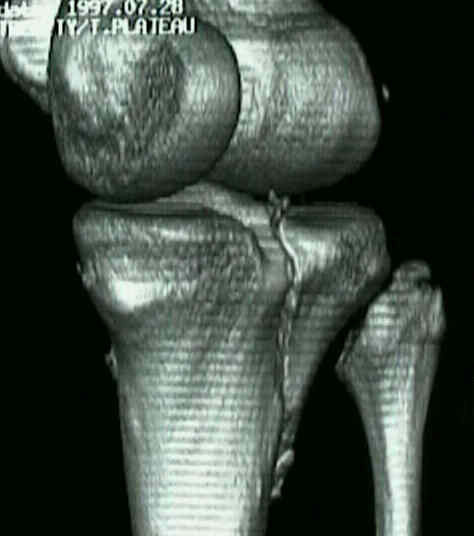
- Discussion: Split Compression / Type II Fractures:
- split fragment from articular surface along w/ depressed area similar to that of local compression frx;
- lateral wedge frx is combined w/ varying deg of depression of adjacent remaining wt bearing portion of lateral tibial plateau;
- depression is usually located anteriorly or centrally;
- wedge frx may vary from a small rim fracture to a frx involving upto 1/3 of the articular surface;
- displacement of frx consists of widening of joint w/ spreading apart of wedge, in combination w/ central depression of lateral plateau;
- mechanism: valgus stress and axial compression forces that 1st cause frx of split fragment & then cause depression frx of part of remaining surface;
- associated injuries:
- look for fracture of fibular head and neck
- most often S.C.F. involves lateral plateau;
- ligament injuries are found in 19% of split compression frx;
- look for widening of medial cartilage space of knee &
- avulsion of bone from medial femoral condyle;
- Radiographs:
- CT scan accurately defines anatomy;
- 20% of SCF have a collat ligament injury;
- look for widening of medial cartilage space;
- avulsion of bone from medial femoral condyle;
- gentle valgus stress may produce deformity of 20 to 25 deg;
- grade depression by measuring vertical distance between lowest point on medial plateau
& lowest depressed frag of lateral plateau;
- depression > 4 mm is sig. & if left untreated results in joint incongruity, valgus deformity,
and a sense of instability;



- Non Operative Rx:
- indicated for frx w/ < 6 mm of articular depression assumming that split fragment is restored to its anatomic position w/ traction;
- split fragments assoc. w/ articular depression of > 6 mm can almost always be reduced, however, articular incongruity will remain &
there will be insufficient support for femoral condyle;
- Traction:
- even if traction fails to yeild an accetable reduction, pt will note pain relief & will be able to begin early ROM;
- Indications for Operative Treatment:
- joint surface is depressed > 1 cm (4 mm in young patients)
- valgus is > than 10 deg;
- closed reduction of split fragment is not maintained;
- associated posterior wedge requires fixation since this significes significant posterior instability;
- Percutaneous Fixation:
- type II frx may often not be amenable to percutaneous fixation because an acceptable reduction of the depressed fragment can be difficult to obtain;
- part of the difficult lies in the fact that the depressed fragment is buried w/ in the plateau and is obsured by the frx lines of split fragment;
- hence the patient should be forewarned about the need for open reduction;
- reduction:
- if the split fragment is depressed, it can be brought out to length with use of a femoral distraction;
- once the fracture fragment has been elevated w/ ligamentotaxis, then the medial or lateral displacement can be corrected;
- reduction is achieved w/ percutaneous applied reduction forceps w/ flourscopic assistance;
- consider applying the reduction forceps eccentrically, and then torque reduction forceps to achieve reduction;
- adequate reduction implies less than 1-2 mm step off;
- depressed fragments: make a small window in the metaphyseal cortex and elevate depressed fragment with a bone tamp;
- fixation:
- percutaneous screws:
- wedge of type I frx of lateral plateau can usually be fixed w/ only cancellous percutaneous lag screws and washers;
- consider 6.5 mm cancellous screws (over washers) which are placed in a triangular position;
- anti-glide screw:
- antiglide screws are typically placed after 1-2 percutaneous lag screws are placed thru the frx fragment;
- antigluide screws (over washers) are placed just distal to the frx edge to prevent distal displacement;
- 4.5 mm cortical screws over washers are typically used;
- references:
- [Comparison study on effectiveness between arthroscopy assisted percutaneous internal fixation and open reduction and internal fixation for Schatzker types II and III tibial plateau fractures].
- Balloon Tibioplasty: A Useful Tool for Reduction of Tibial Plateau Depression Fractures
- Percutaneous Screw Fixation of Tibial Plateau Fractures.
- Closed reduction and percutaneous screw fixation for tibial plateau fractures
- Indirect reduction and percutaneous screw fixation of displaced tibial plateau fractures.
- Open Surgical Treatment: (Synthes Products)
- PreOp Planning
- most important step in reconstruction of any intra articular frx, is to expose the fracture w/o devasclarizing the fragments;
- Treatment Plan:
- open reduction;
- elevation of the depressed plateau;
- bone grafting of metaphysis;
- fixation of the fracture with cancellous screws
- butress plating of the lateral cortex;
- Position:
- for optimal exposure, consider supine position, w/ a bolster under thigh, & table broken so that the knee is flexed 90 deg;
- this position allows increased exposure submeniscally;
- Surgical Approach:
- consider a longitudinal lateral parapatellar approach;
- elevate anterior compartment muscles off proximal tibia, exposing tibial flare and split frx;
- trace frx is to joint line and enter joint thru transverse sub-meniscal interval;
- if needed, transect attachment of anterior horn of meniscus;
- elevate meniscus superiorly to expose intra-articular frx segment;
- Exposure of Depressed Segment:
- split frx is hinged open anteriorly to expose depressed joint surface;
- this surface is elevated to appropriate level & defect is filled w/ or local cancellous bone or allografts;
- apply small impactor from below to disimpact and elevate depressed segment;
- apply bone graft from below;
- elevated segment may be supported w/ K wires (consider biodegradable);
- ref: Inside out rafting K-wire technique for tibial plateau fractures
- Reduction:
- consider use of tenaculum or pelvic reduction clamp across both plateau to generate compression;
- Implants: (Synthes Products)
- at this point, the frx has essentially been turned into a type I frx;
- w/ minimal comminuation and good bone stock, consider 6.5 mm cancellous screws w/ or w/o washers;
- if cannulated screws are used, these are inserted over K wires;
- if split fragment is not comminuted, 2 or 3 cancellous screws are inserted parallel to & > 1 cm distal to articular surface;
- an additional, cortical anti-glide scrw w/ washer is inserted distally;
- in older patients, w/ osteoporotic bone, lag screws alone cannot prevent redisplacement of fragments; (need butress plate);
- a comminuted frx, requires an L or T shaped buttress plate; another indication, for butress plating is assoc subcondylar frx;


- Post Operative Care and Compications:
- Loss of Reduction of split frag is main complication of Rx in split compression frx;
- this is found more commonly with closed treatment;
- w/ percutaneous IF, a cast brace is used until frx healing is complete;
- w/ use of a butress plate to assure rigid fixation, external support is not required postoperatively
Indirect Reduction and Percutaneous Screw Fixation of Displaced Tibial Plateau Fractures.
Split depression tibial plateau fractures: a biomechanical study.
Combined Arthroscopic Treatment of Tibial Plateau and Intercondylar Eminence Avulsion Fractures