- AP and Lateral:
- radiographs are assessed for frx locations, displacement, alignment;
- lateral plateau is convex from front to back & side to side, whereas medial one is concave;
- lateral plateau is higher than medial one, which indicates amount of plateua depression;
- upper tibial articular surface nl inclines posteriorly from 10-15 deg & hence by angling AP beam caudally 15 deg will give better views;
- on standard x-ray of knee, plateau appears ellicptical in shape, & posterior edge is represented by lower of two lines;
- consider radiographs of contra-lateral plateau for templating;
- role of the fibula in plateau frx:
- reference:
- Segond fracture combined with tibial plateau fracture.
- Oblique: internal and external
- helpful in determining the amount and location of depression;
- Stress View: to document ligamentous laxity;
- according to Rasmussen, major indication for Rx is not measure of depression of fragment or articular surface but presence of varus or
valgus instability of 10 deg or more w/ knee flexed 20 deg;
- Traction Radiographs:
- may be useful in more complex frx;
- Tomograms:
- consider ordering both the AP and the Lateral Tomographic cuts;
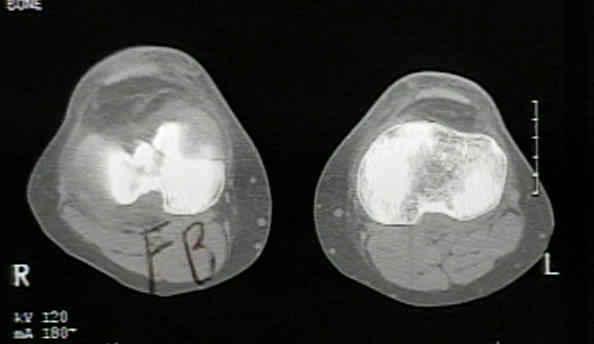
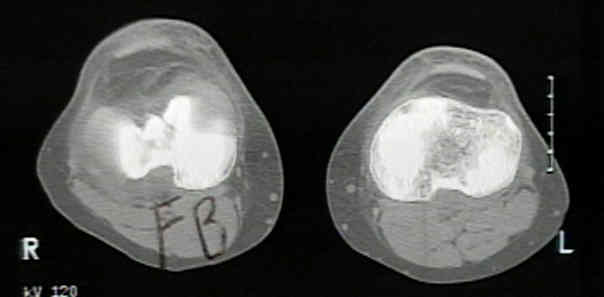
- CT:
- consider either 1.5 mm fine axial cuts w/ coronal reconstructions (for pts who cannot bend their knees, or 5 mm axial cuts along with 3
mm direct coronals for patients who can bend their knees;
- defines the size of the fracture
- depression of the fragments
- position of the lateral wedge and the remaining intact bone;
- comminution of the fracture, particularly the depressed fragment;
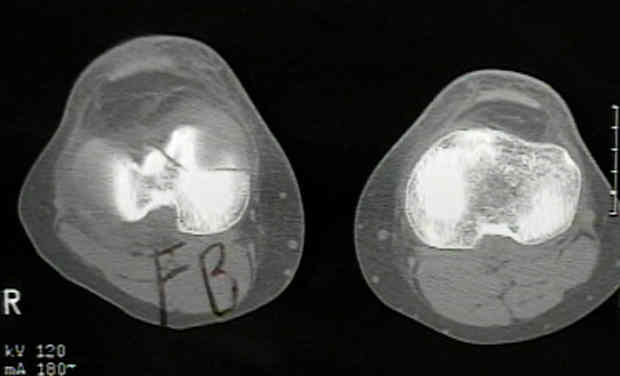
- case example:
- at first glance, the AP radiograph does not show the lateral sided depression, but a closer look shows a subchondral density well below the joint line;
- seeing that the radiograph can under-represent the amount of the depression, a CT scan should generally be obtained


- MRI
- references:
Tibial plateau fractures: evaluation with MR imaging.
Computerised axial tomography for tibial plateau fractures.