

- See: Phalangeal Injury Menu:
- Discussion:
- fractures of the proximal phalanx are potentially the most disabling fractures in the hand;
- direct blows tend to cause transverse or comminuted frx, where as twisting injury may cause oblique or spiral fracture;
- proximal fragments are usually flexed by intrinsics while distal fragments are extended due to extrinsic compressive forces;
- most frequent complication of this type of fracture is extensor mechanism adhesions with subsequent loss of motion;
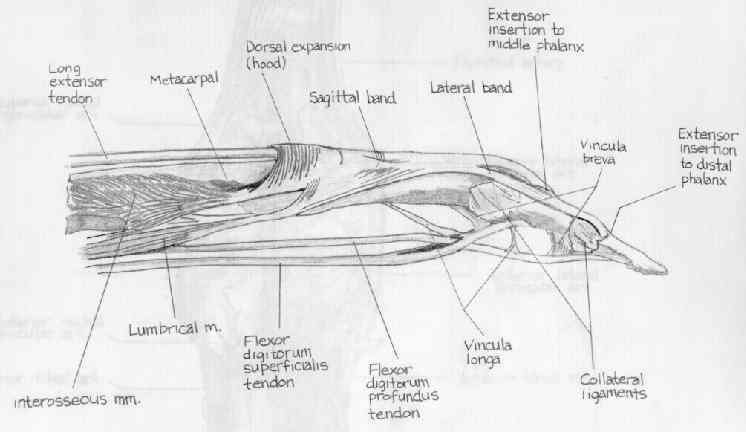
- it is also important to note that that periosteum of proximal and the middle phalanges forms the dorsal wall of fibroosseous tunnel in which flexor tendon glides;
- consequently any frx of these phalannges interrupts continuity gliding surface of the flexor tendon sheath;
- angulation & deforming forces:
- unstable frx of the proximal phalanx typically present w/ volar angulation (usually about 30 deg);
- proximal fragment is flexed by the bony insertion of interossei into base of the proximal phalanx;
- although there are no tendons inserting on the distal fragment, it tends to be pulled into hyperextension by the central slip acting on the base of the middle phalanx;
- once stability of proximal phalanx is lost, there is an accordion like collapse at fracture site, aggravated by further pull on extensor hood by extrinsic muscles;

- Pediatric Proximal Phalanx Frx:
- extra-octave frx:
- transverse frx at neck of proximal phalanx:
- common in children - "booby - trap - fracture"
- angulation is between 60 and 90 deg. (apex volar);
- reduction is easy to obtain but difficult to maintain;
- accetable reduction:
- older children will not be able to remodel beyond 20 deg;
- more than 10 deg of final angulation will interfere with function;
- as pointed out by Coonrad and Pohlman (1969), children younger than age 10 yrs can remodel up to 30 deg;
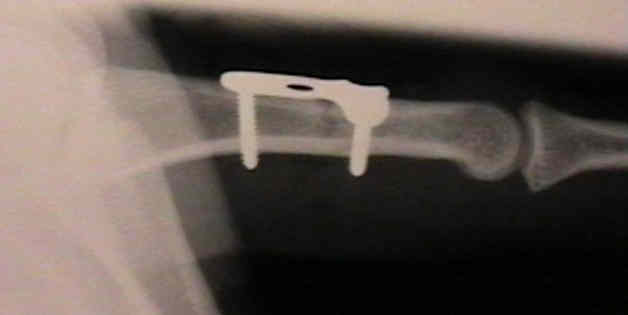
- Impacted fractures in the proximal portion of the proximal phalanx of the finger.
- Types of Adult Proximal Phalanx Fracture:
- Base of Proximal Phalanx:
- Condylar Fracture:
- usually there is frx of single condyle, resulting in disruption of the joint and angular deformity of the finger;
- requires internal fixation and exact anatomic restoration of articular surface;
- Spiral - Oblique Frx: is inherently unstable, and requires internal fixation;
- Transverse Frx:
- surface of midshaft is small and composed primarily of cortical bone and therefore frx involving mid-shaft, heal slowly;
- from 5-6 weeks of immobilization may be needed before adequate healing;
- Exam:
- malrotation is a common problem and can be examined for by checking
for the normal cascade in finger flexion with the tips of the
fingers pointing toward the proximal portion of the scaphoid;
- Acceptable Reduction:
- no rotational deformity can be accepted;
- no more than 10 deg of angulation should be accepted in any plane;
- if allowed to unite with 25 deg or more of volar angulation, digital motion will be impaired, as extensor mechanism becomes shortened leading to
a loss of full extension at the PIP joint;
- malreduction will cause loss of equilibrium between flexor and extensor tendons;
- Non Operative Treatment of Stable Fractures
- Indications for Operative Treatment:
- volarly angulated frx;
- condylar fracture:
- spiral - oblique frx: is inherently unstable, and requires internal fixation -
- supra-condylar fractures: tend to have severe volar angulation;
- frx dislocation of PIP Joint:
- phalangeal head fractures:
- w/ extensively comminuted metacarpal head fractures, treat closed & hold in appropriate position and begin ROM at 14 days;
- Operative Anesthesia:
- 2% mepivacaine (carbocaine);
- consider wrist block (median, radial, ulnar, and ulnar dorsal sensory), since this allows the patient to actively ROM the fingers following frx fixation;
- Operative Treatment Options:
- screw fixation:


- interosseous wires
- percutaneous intramedullary K wire:
- indicated for transverse - unstable frx of base, shaft, and neck;
- transverse pinning technique:
- indicated for spiral - oblique frxs:
- cross pinning technique:
- K wires should never cross at the fracture site, since this will cause rigid distraction;
- K wires should cross either proximal or distal to the fracture and gain firm anchorage in the proximal and distal metaphysis;
- plate fixation:
- dorsal midline approach:
- indicated for fractures located with in the proximal 2/3 of the proximal phalanx;
- make a dorsal longitudinal incision which gently curves to over one side of the phalanx;
- split the extensor mechanism down the middle;
- carefully preserve the periosteum (which will be repaired over the plate):
- Chamay approach:
- indicated for fractures over the distal 1/3 of the proximal phalanx;
- make a dorsal longitudinal skin incision over the phalanx;
- make a distally based "V shaped" flap incision into the extensor mechanism;
- this allows the central slip to be reflected distally and does not interfere with the lateral bands;
- approach to shaft:
- spliting central extensor tendon longitudinally;
- dissecting the interval between lateral band and extensor tendon;
- periosteum is elevated as a long, wide flap;
- periosteum protects extensor mechanism from metal implants;



- Complications: Adhesion Formation: (see: flexor tenolysis)
- adhesions form if part is immobilized because the wound in sheath and wound in the tendon grow together;
- if part is kept mobile, they heal separately, and function is more likely to be restored;
- collagen tensile strength across the repair is not sufficient to permit active loading for 4-5 weeks
- on physical exam, the patient will demonstrate loss of active flexion, but relative maintenance of active extension and maintenance of passive flexion;
- severe adhesion formation is managed with tenolysis
Treatment principles for proximal and middle phalangeal fractures.
Articular fractures of the digits: a prospective study.
A prospective study of 245 open digital fractures of the hand.
Role of antibiotics in open fractures of the finger.
Distal unicondylar fractures of the proximal phalanx.
An analysis of proximal phalangeal fractures.
A comparative mechanical analysis of plate fixation in a proximal phalangeal fracture model.
Complications in phalangeal and metacarpal fracture management. Results of tenolysis.
Tenolysis and capsulectomy after hand fractures.
Volar Plating for Intra-Articular Fracture of the Base of the Proximal Phalanx