



- a common benign but locally aggressive lesion of unknown etiology;
- occurs chiefly in men between 20-50 yrs (after epiphyseal closure);
- tumor is expansile lytic lesion that involves the epiphysis & metaphysis;
- tumor may enlarge to occupy most of epiphysis & adjacent metaphysis;
- tumor may erode & penetrate subchondral bone, articular cartilage, & cruciate ligaments;
- location:
- epiphysis of distal femur, proximal tibia, & distal radius;
- other sites: fibula, sacrum, proximal humerus, & distal tibia;
- can occur in bones of pelvis, particularly ilium near SI joint and sacrum;
- spine:
- usually located in vertebral body;
- radiolucent lesion in vertebral body of a young patient is likely to be GCT;
- ref: Giant Cell Tumor of the Pelvis and Sacrum: 17 Cases and Analysis of the Literature.
- staging:
- stage I:
- benign latent giant cell tumors;
- no local agressive activity;
- stage II:
- benign active GCT;
- imaging studies demonstrate alteration of the cortical bone structure;
- stage III:
- locally aggressive tumors;
- imaging studies demonstrate a lytic lesion surrounding medullary and cortical bone;
- there may be indication of tumor penetration through the cortex into the soft tissues;
- prognosis:
- tumors w/ malignant stroma tend to behave in malignant fashion;
- lesions that appear benign may metastasize;
- 5% of pts will have pulmonary metastases (2% risk of benign pulmonary metastasis in all cases and 6% risk in recurrent cases);
- tumor is considered benign if pulmonary lesions are histologically benign;
- pulmonary lesions may be cured w/ surgical resection;
- GCT involving the distal radius may be more aggressive than in other locations;
- differential dx:
- non ossifying fibroma;
- aneurysmal bone cyst;
- histoplasma
- Histoplasma Osteomyelitis Simulating Giant-Cell Tumor of the Distal Part of the Radius: A Case Report.
- hyperparathyroidism:
- may produce brown tumors that are radiographically & histologically similar to giant cell tumor of bone, w/ the exception
that brown tumors tend to be diaphyseal in location;
- unlike brown tumors, serum Ca is normal in GCT;
- Clinical Manifestations:
- pts report deep, persistent intraosseous pain that mimics an internal derangement of the knee.
- pathologic frx or reactive knee effusioin is initial symptom in about 1/3 of pts;
- Radiographic Features:
- well-defined lytic lesion that involves the metaphysis and epiphysis (typical of a giant cell tumor);
- CT Scan:
- helps determine is extact amount of cortical destruction and helps determine the optimal location of the cortical window;
- Bone Scans:
- bone scans may show decreased radioisotope uptake in the center of lesion (doughnut sign); (also found w/ ABC);
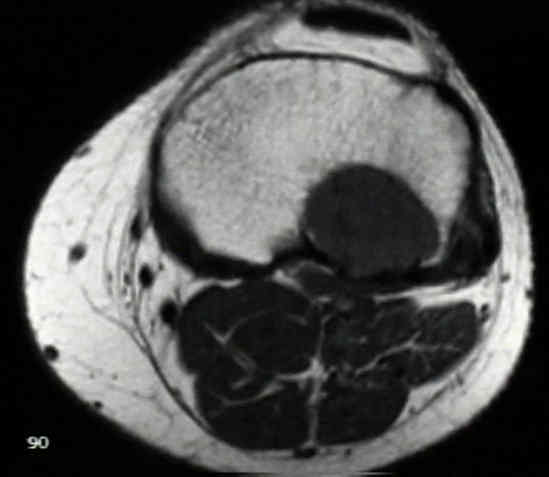
- MRI:
- help determine determine extent of tumor destruction;
- may be indicated when the tumor has eroded thru the cortex and allows determination of whether concomitant neurovascular
structures are involved;
- may help evaluate subchondral penetration;



- Histologic Studies;
- Treatment:
- due to proximity to articlar cartilage, excision of GCT of bone is difficult;
- because intralesional excision of GCT tends to leave tumor cells behind, past attempts of excision had been asociatted w/ high
recurrance rate (40%);
- GCT involving the distal radius may be more agressive that GCT in other locations;
- prior pathologic fracture should be allowed to heal before surgery is attempted;
- ref: Giant Cell Tumor With Pathologic Fracture: Should We Curette or Resect?
- Stage 1 or 2 Lesions:
- intra-lesional excision is treatment of choice;
- excision is facilitated by making a large cortical window;
- window must be large enough to allow complete access to every corner of the intra-osseous lesion;
- high speed burr is used to complete the excision, with care taken to remove 5 mm of normal bone surrounding the lesion;
- at completion of procedure (which usually involves placement of cement or bone graft in the cavity), window is replaced w/
bone graft or w/ bone graft substitute;
- note that in areas such as the distal ulna or fibula, en bloc excision is preferred over currettage because there is minimal functional
consequences of en bloc exision;
- motorized burr and cautery are used to complete and excision the excision;
- when motorized burr is used to debride the subchondral bone, the joint cartilage should be irrigated w/ chilled saline;
- Blackley, et al (1999), the authors followed 59 patients who underwent curettage and bone grafting of GCT lesions;
- 12% had a local recurrence (and all but one of these patients responded to revision currettage and/or soft tissue resection);
- low recurrence rate was due to meticulous debridement of GCT tissue which included use of a high speed burr;
- ref: Treatment of giant-cell tumors of long bones with curettage and bone-grafting.
- adjunctive measures:
- use of phenol, polymethacrylate, and liquid nitrogen;
- phenol can be extremely toxic, and if used at all, its concentration should be limited to 5%;
- these work by increasing the zone of necrosis at periphery of excision;
- cement:
- heat generated from the polymerization reaction may kill tumor cells 0.5 mm in cortical bone and 2 mm in cancellous bone;
- as reported by O'Donnell, et al (1994) the use of cement did not appear to improve the results as compared to historic
controls with a 25% recurrence rate w/ long term follow up;
- barium impregnated cement allows for accurant determination of local recurrance;
- cement provides mechanical support following curretage and does not appear to affect cartilage when placed in the
subchondral region;
- when cement is applied beneath subchondral cartilage, joint should be irrigatted w/ chilled saline, inorder
to protect cartilage;
- Recurrence of giant-cell tumors of the long bones after curettage and packing with cement.
- liquid nitrogren:
- may cause excessive tissue necrosis, extending into normal tissue;
- bone grafting:
- Supplemental Bone Grafting in Giant Cell Tumor of the Extremity Reduces Nononcologic Complications.
- Recurrent or Stage 3 Lesions:
- this category includes frx w/ major pathologic frx, articular or cortical penetration by the tumor;
- en bloc excision w/ wide margin along w/ appropriate reconstruction;
- en bloc excision involves removal of one side the joint, necessitating a major limb reconstructive procedure (often w/ allografts);
- chemotherapy:
- Denosumab, a Potential Alternative to the Surgical Treatment of Distal Radius Giant Cell Tumor of Bone: Case Report
- radiation therapy
- traditionally XRT is avoided because of the possibility of malignant degeneration of the tumor;
- in the report by Chakravarti, et al JBJS 1999, 20 patients underwent a single course of megavoltage radiation (40-70 gray
administered at 1.8 to 2.0 gray per fraction with an average total duration of treatment of 5-7 weeks)
- after a median duration of follow-up of 9.3 years, the tumor had not progressed in seventeen of the twenty patients;
- no radiation-induced tumors were observed in our series;
- authors note that the results of XRT were comparable to published efficacy of surgical resection;
- references:
- Megavoltage Radiation Therapy for Axial and Inoperable Giant-Cell Tumor of Bone.
- pulmonary metastasis:
- 5% of pts will have pulmonary metastases;
- tumor is considered benign if pulmonary lesions are histologically benign;
- pulmonary lesions may be cured w/ surgical resection;
- references:
- Pulmonary metastasis of benign giant cell tumor of bone. Six histologically confirmed cases, including one of spontaneous regression.
- Giant-cell tumor of bone with pulmonary metastases.
- Giant-cell tumor of bone with pulmonary metastases. Six case reports and a review of the literature.
- Benign metastasizing giant-cell tumor of bone. Report of three cases and review of the literature.
- Metastases from histologically benign giant-cell tumor of bone.
- Treatment Methods by Anatomic Location:
- GCT of radius:
- Distal ulnar translocation in the treatment of giant-cell tumors of the distal end of the radius.
- Fibular reconstruction for giant cell tumor of the distal radius.
- Giant-cell tumors in the distal end of the radius. Treatment by resection and fibular autograft interpositional arthrodesis.
- Giant-cell tumor of the radius treated by massive resection and tibial bone graft.
- Giant cell tumor of the distal radius.
- The treatment of giant-cell tumors of the distal part of the radius.
- Giant-cell tumor of the distal forearm
- GCT of pelvis and sacrum:
- The treatment of sacral giant-cell tumours by serial arterial embolisation
- Conservative surgery for giant cell tumors of the sacrum. The role of cryosurgery as a supplement to curettage and partial excision.
- Giant cell tumor of the sacrum.
- Treatment of Giant-Cell Tumor of the Pelvis.
- Surgical treatment of giant cell tumors of the pelvis.
Giant-cell tumor of bone - I
Giant-cell tumor of bone - II
Secondary malignant giant-cell tumor of bone. Clinicopathological assessment of nineteen patients.
Reconstruction of musculoskeletal defects about the knee for tumor.
CO2 laser cauterization of giant-cell tumor margins.
Giant-cell tumor of bone in skeletally immature patients.
Multicentric giant-cell tumor of bone.
Secondary malignant giant-cell tumor of bone. Clinicopathological assessment of nineteen patients.
Total spondylectomy for removal of a giant-cell tumor in the eleventh thoracic vertebra. Stener B: Spine 1977;2:197-201.
Giant-cell tumor of bone. An analysis of 218 cases.
Radiology of giant cell tumors of bone: computed tomography, arthro-tomography, and scintigraphy.
Giant-cell tumours of the spine.
The Use of a Bone Allograft for Reconstruction after Resection of Giant-Cell Tumor Close to the Knee.
Intralesional excision compared with en bloc resection for giant-cell tumors of bone.
Favorable results of acrylic cementation for giant cell tumors.
Recurrence of giant-cell tumors of the long bones after curettage and packing with cement.
Giant cell tumours of the hand.
Radiation therapy for giant cell tumors of bone.
Giant Cell Tumor of the Pelvis and Sacrum: 17 Cases and Analysis of the Literature.
Results of Giant Cell Tumor of Bone Treated With Intralesional Excision.
Bisphosphonates May Reduce Recurrence in Giant Cell Tumor by Inducing Apoptosis.
Does Curettage without Adjuvant Therapy Provide Low Recurrence Rates in Giant-Cell Tumors of Bone?
Impact Severity of Local Recurrence in Giant Cell Tumor of Bone.
Intralesional Curettage for Grades II and III Giant Cell Tumors of Bone.
CASE REPORT: Iatrogenic Seeding of a Giant Cell Tumor of the Patella to the Proximal Tibia.
Treatment of giant-cell tumors of long bones with curettage and bone-grafting