

- night stick fracture: mechanism: direct trauma w/ forearm used to block blow
- stable frx:
- diplaced < 50% = Stable;
- periosteum & interosseous membrane are intact & act as restraint to rotation;
- unstable fracture:
- displaced > 50% or > 10-15 deg angulation;
- angulation or displacement towards the interosseous membrane is poorly tolerated;
- periosteum and interosseous membrane disrupted;
- associated injuries: radial head frx or dislocation (see Montegga frx)
- non operative treatment:
- indicated for fractures in the distal 2/3 of the forearm with less than 10-15 deg angulation and more than 50% to 75% fracture opposition;
- well fitted forearm cast or brace which does not interfere with wrist or elbow motion;
- expect 50% reduction of forearm pronation or supination while in the brace;
- references:
- Treatment of ulnar fractures by functional bracing.
- The isolated fracture of the ulnar shaft. Treatment without immobilization.
- Bracing of stable shaft fractures of the ulna.
- Early mobilization of isolated ulnar-shaft fractures.
- Isolated ulnar shaft fractures. Comparison of treatment by a functional brace and long-arm cast.
- Treatment of isolated ulnar shaft fractures with prefabricated functional fracture braces.
- The isolated fracture of the ulnar shaft. Treatment without immobilization.
- surgical options:
- see: approach to the ulna and plating techniques;
- open fractures: (see Gustillo classification)
- open fractures should be treated as an emergency, but fixation may be delayed upto 24 hrs;
- immediate ORIF in grade I, II, and IIIa fractures can have good results (low infection rate);
- autogenous bone grafting can be carried out early for grade I and II fractures (if needed);
- grade IIIb and IIIc fractures had poor results;
- these fractures were serially debrided until judged clean, only at which time was bone grafting performed;
- despite these measures, infections may occur in upto 3/4 of these patients;
- wound closure:
- some surgeons will close surgical incisions, where as, traumatic wounds are left open and are closed by delayed suture at a second or third look debridement;
- 2 days of antibiotics should follow each wound debridement;
- consider antibiotic bead pouch between debridements;
- references:
- Immediate internal fixation of open fractures of the diaphysis of the forearm.
- The necessity of acute bone grafting in diaphyseal forearm fractures: a retrospective review.
- The treatment of isolated fractures of the distal ulna.
- Isolated ulnar shaft fractures. Retrospective study of 46 cases.
- Non-union of the isolated fracture of the ulnar shaft in adults.
- Early mobilization of isolated ulnar-shaft fractures.
- Isolated ulnar shaft fractures. Comparison of treatment by a functional brace and long-arm cast.
- Treatment of isolated ulnar shaft fractures with prefabricated functional fracture braces. 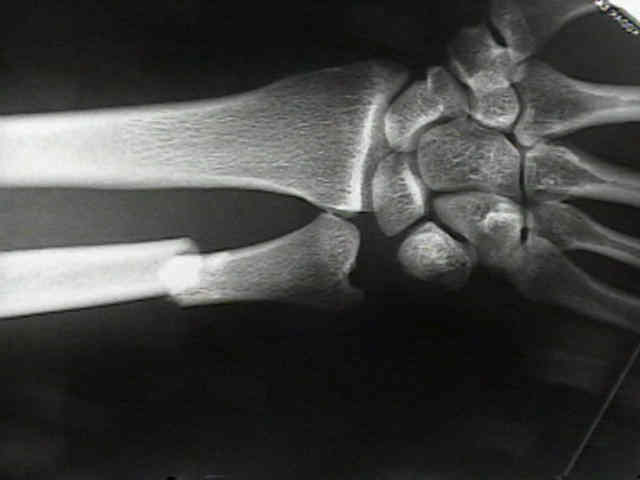
- frx complications:
- non union: approx: 5%;
- ulnar carpal abutment:
- references:
- Non-union of the isolated fracture of the ulnar shaft in adults.
- Atrophic nonunions of the proximal ulna.