

- See:
- Safe Zone of Pin Insertion
Wires Insertion Techniques
- Wire Characteristics:
- in general 1.5 to 1.8 mm wires need no incision or drill sheath, but larger, 2.0 wires may be inserted w/ sheath through incision;
- larger diameter wires will increase stiffness of the frame;
- generally, the 1.8 mm wire is used for the humerus, tibia, and femur;
- in smaller patients 1.5 mm wires should be used;
- whether a ring or unilateral fixator is used, there is some evidence that a better regenerate is formed with the use of titanium half pins rather than transfixation wires;
- ref: Limb lengthening by callus distraction (callotasis).
- wire tips: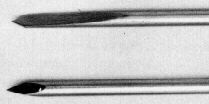
- trocar tip is used for metaphyseal bone;
- bayonet tip is used for diaphyeal bone;
- it produces a hole of slightly larger diameter than that of the wire;
- these wires have a special cutting tip so that predrilling is not required;
- olive wires:
- used to assist in indirect reduction;
- wire is inserted w/ goal of applying tension to the ball inorder to pull the fracture into alignment;
- olive wires require a small incision of skin only;
- cautions: olive wires may tend to cut thru cancellous bone, resulting in loss of reduction;
- note: when olive wires are inserted they should be marked in order that the correct end will be pulled out bone at the time of fixator removal;
- titanium pins:
- see: properties of titanium;
- may have a lower incidence of infection than stainless steel;
- more flexible than stainless steel, however, use of 6 mm pin brings pin stiffness up to par w/ stainless steel;
- Stability of Construct / Position of Pins:
- see safe zone of pin insertion for tibial frx;
- it is safest to insert pins from the more vulnerable side to the less vulnerable side;
- wire diameter and wire tension are important factors in frame stability;
- large fragments require 2 levels of fixation w/ 2 wires (or one wire and one half pin) at each level of fixation;
- short fragments may be fixed w/ one ring w/ a drop wire (in which case the insertion pin is offset from the ring by 1-2 cm);
- stability is increased by having pins transfix bone at right angles at each level within anatomic constrainst;
- if pins are to be crossed at the same level, it is prudent to insert one pin above the ring and another below the ring;
- Pin Attachment to Frame:
- never bend a pin to meet a frame, but instead, either remove and reinsert the pin, or use spacers to attach the pin to the fixator;
- wires are attached to ring using either cannulated or slotted fixation bolts, the choice depending on which bolt minimizes wire bending;
- w/ one wrench holding the fixation bolt stationary, the remaining wrench tightens the fixation nut;
- Wire Tensioning:
- tensioning is performed thru slotted wire fixation bolt;
- tensionig is carried out by fixing one end of the wire and tensioning the other wire;
- frame stiffness will be increased by increasing wire tension, which has the effect of decreasing motion at the fracture site;
- note when drop wires are used, the tensioner will not have the ring to act as a counter post;
- in this situation, introduce a hexagonal post between the drop wire's fixation bolts and then tensioner (and then apply the tensioner in the usual way);
- wires are tensioned between 100-130 kg of force;
- exceptions:
- drop wire: 50 to 80 kg;
- single wire on a ring 100 kg;
- olive wire: 100 kg;
- Post Op:
- it is essential to check periarticular wires for signs of inflammation or superficial infection, in order to avoid possible septic arthritis;
- it is essential that the wire tension be checked, since loss of tension will result in loss of frame stability
The use of wires and pins. Green SA. Techn Orthop. 1990;5:19-25.