

(see also: Achilles Tendonitis)

Discussion
- ruptures typically occur after age 30, more often in people beyond middle age;
- rupture at musculous tendinous junction occurs most often in young people, but ruptures near the calcaneus also occur;
- inciting event may be related to atrophy of the soleus muscle, and commonly occur in weekend athletes;
- in 5-33% of patients there will be a prodromal incident of pain several days beforhand;
- mechanism usually involves eccentric loading on a dorsiflexed ankle with the knee extended (soleus and gastroc on maximal stretch);
- unlike flexor tendons in the hand, the Achilles tendon has no true synovial sheath, but rather is covered only by a paratenon;
- hence, exogenous healing (from synovial fluid) would not be expected to occur;
inciting causes
- consider systemic conditions such as gout or hyperparathyroidism (esp with pure avulsion injury);
- inquire about previous steroid injections / injections of steroids into or around the Achilles tendon may provoke rupture and should generally be avoided;
- flouroquinolones may also contribute to tendon rupture;
Exam Findings »
Radiographic Studies
Non Operative Rx »
- Operative versus nonoperative treatment of acute Achilles tendon ruptures: a multicenter randomized trial using accelerated functional rehabilitation.
- Ruptures of the tendo achillis. An objective assessment of surgical and non-surgical treatment.
- Surgical and non-surgical treatment of Achilles Tendon rupture. A prospective randomized study.
- Achilles tendon rupture: an alternative treatment.
- Practice patterns in the care of acute Achilles tendon ruptures is there an association with level I evidence?
- Treatment of acute Achilles tendon rupture with a standardised protocol
- Functional weight-bearing mobilization after Achilles tendon rupture enhances early healing response: a single-blinded randomized controlled trial.
Operative Repair
discussion
- most indicated in a younger patient w/ a clinically displaced rupture;
- may allow earlier return to sports, earlier return of muscle power, and a lower re-rupture rate as compared to non operative
- main complication is wound slough;
positioning
- place the tourniquet on the leg in the supine position, before turning the patient prone (its difficult to place the tourniquet in the prone position);
- before prepping, note the resting equinus position of the uninjured leg (and attempt to reproduce this equinus position during surgery);
- if a surgical assistant is not available, position the patient so that the dorsum of the forefoot remains on the table (not dangling off the table), so that the foot can be held in equinus during the tendon repair;
incision
- longitudinal incision is made just medial to achilles tendon;
- a medially placed incision may be less likely to slough from the pressure that the repaired tendon exerts on the overlying skin;
- additionally a medially placed incision is less likely to develop postop adhesions;
- a laterally placed incision may injure the sural nerve and the lesser saphenous venous plexus;
para-tenon
- w/o creating a flap, the incision is carried down to the para-tenon;
- some surgeons will attempt to cut the paratenon straight over the tendon (as opposed to the the medial side in line with the incision);
evaluate tendon defect
- identify the level of the rupture of the Achilles tendon;
- attempt to identify the plantaris tendon;
- mobilize the proximal Achilles tendon by sweeping a finger circumferentially aroung the tendon border (thus breaking up adhesions);
- using non-traumatic clamps, match the ends of the ruptured tendon to achieve optimal length;
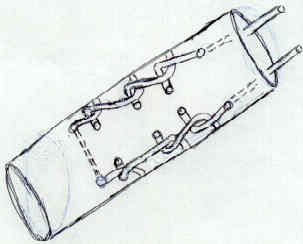
suture repair
- coronal running horizontal suture repair;
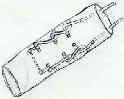
- consider a simple running horizontal matress stitch made in the coronal plane (medial to lateral) so that none of the sutures face the surgical incision;
- in the case of wound break down, the core suture will not be exposed lessening the chance of infection;
- Krachow whip stitch, along each tendon edge, using No 5 Tycron or Ethibond on a Non Cutting Needle;
- running "Tajima stitch" which provides good strength but does not create the overlying prominent sutures;
- Becker suture technique:
- Singer et al (1998), the core suture technique was the most important element in establishing both strength and stiffness of the repair;
- repair consists of criss-crossing running suture using a double armed needle;
- sutures should be placed 0.75 cm from the cut edge of the tendon;
- as noted in the report by Howard et al. (1997), the MGH tendon repair technique (crossing running suture repair) was signficantly more resistant to gap formation than the Bunnel or the Krackow technique;
- MGH tendon repair has superior suture purchase which is probably related to superior resistance to gap formation;
- tendon edges are approximated together w/ non traumatic clamps, before the suture arms are brought thru the tendon edges;
- before tying the sutures, note the degree of equinus in the opposite ankle (it is essential to optimize tension);
- each side is tied simultaneously to optimize tendon oposition;
- following the core suture repair, run a 2-0 Vicryl suture on a non-cutting needle to further oppose the irregular edges of the ruptured tendon;
- references:
- Biomechanical analysis of four-strand extensor tendon repair techniques
- Core weave versus Krackow technique for Achilles tendon repair: a biomechanical study
- Use of the Taguchi method for biomechanical comparison of flexor-tendon-repair techniques to allow immediate active flexion. A new method of analysis and optimization of technique to improve the quality of the repair.
- The "Giftbox" repair of the Achilles tendon: a modification of the Krackow technique
- [Aseptic drainage associated with polyglactine sutures used for repair of Achilles tendon ruptures].
- [Tendon holding capacities of the suture materials used in repairing Achilles tendon rupture].
- Biomechanical testing of epitenon suture strength in Achilles tendon repairs.
- Cyclic loading of Achilles tendon repairs: a comparison of polyester and polyblend suture
fascial augmentation
- gastrocnemius aponeurosis:
- make rectangular 1-2 cm wide by 8 cm long flap from proximal tendon and gastroc aponeurosis which is raised to with in 3 cm of rupture site;
- immediately beneath the gastroc fascia, the surgeon will note the soleus muscle;
- proximal flap edge is then flipped distally across the repair site and sutured down;
- the fascial defect is closed with interrupted sutures;
- stated advantageous include less adhesion formation and a stronger repair;
- make rectangular 1-2 cm wide by 8 cm long flap from proximal tendon and gastroc aponeurosis which is raised to with in 3 cm of rupture site;
- plantaris tendon augmentation:
- can be used to augment the repair by weaving it across the repair site;
- it can be left attached either proximally or distally;
- alternatively plantaris tendon can be fanned out to make a 2.5 cm membrane that is then sutured around the repair site;
- attempt to close paratenon, especially over the tendon repair site; this is important both for healing and prevention of adhesions;
post operative care »
- references:
- Repair of the calcaneal tendon. An improved technique.
- Repair of Achilles tendon ruptures with Dacron vascular graft.
- A flap augmentation technique for Achilles tendon repair. Postoperative strength and functional outcome.
- A new treatment of ruptured Achilles tendons. A prospective randomized study.
- Surgical repair of Achilles tendon ruptures.
- Separation of tendon ends after Achilles tendon repair: a prospective, randomized, multicenter study.
- A combined open and percutaneous technique for repair of tendo Achillis. Comparison with open repair.
- Repair of acute Achilles tendon ruptures.
- An analysis of skin perfusion over the achilles tendon in varying degrees of plantarflexion
- Early Weightbearing and Ankle Mobilization after Open Repair of Acute Midsubstance Tears of the Achilles Tendon.
Complications
Deep Infection and Wound Breakdown
(see also: prevention of infection)
- Rerupture and Deep Infection Following Treatment of Total Achilles Tendon Rupture
- One-stage treatment of deep infection following repair of Achilles tendon rupture with flexor hallucis longus transfer
- Treating the acute disruption of the Achilles tendon: the nonoperative option
- Wound complications after open Achilles tendon repair: an analysis of risk factors.
- Wound Complications from surgeries pertaining to the Achilles tendon: an analysis of 219 surgeries
- Late intratendinous abscess of the Achilles tendon complicating surgical repair: a case report
- One-stage treatment of deep infection following repair of Achilles tendon rupture with flexor hallucis longus transfer
- Complications of the treatment of Achilles tendon ruptures
Wound Vac Therapy »
(followed by STSG)
- [Vacuum therapy for deep wound infection after Achilles tendon repair].
- [V.A.C.-therapy: a treatment option for wound healing complications after achilles tendon reconstruction].
- Treatment of the exposed Achilles tendon using negative pressure wound therapy: a case report.
- The use of negative-pressure therapy and skin grafting in the treatment of soft-tissue defects over the Achilles tendon.
- Outcome of skin graft versus flap surgery in the salvage of the exposed achilles tendon in diabetics versus nondiabetics.
- Use of External Ring Fixation in a Full-Thickness Achilles Wound: A Case Report
Chronic Tear
- in the report by Pintore E , presented the results of a single-center, single-surgeon study in 59 patients with a fresh (4 women and 23 men; mean age, 43.6 ± 8.8 years) or a neglected (1 woman and 21 men; mean age, 41.3 ± 7.4 years) Achilles tendon rupture;
- patients with a neglected rupture received the tendon of the peroneus brevis as an autologous graft;
- patients were generally satisfied with the procedure, but those with a neglected rupture tended to have a greater postoperative complication rate, greater loss of isokinetic strength variables at high speeds, and greater loss of calf circumference;
- patients w/ neglected rupture are at a slightly greater risk of postoperative complications, and their ankle plantar flexion strength can be reduced;
- references:
- Peroneus Brevis Tendon Transfer in Neglected Tears of the Achilles Tendon.
- Chronic rupture of the Achilles tendon: a new technique of repair.
- Neglected rupture of the Achilles tendon. Treatment by V-Y tendinous flap.
- Late versus early repair of Achilles tendon rupture. Clinical and biomechanical evaluation.
- Flexor hallucis longus transfer for repair of chronic achilles tendinopathy.
- Technique tip: avoiding wound complications after neglected Achilles tendon repair using a tissue expansion technique
- Peroneus Brevis Tendon Transfer for Reconstruction of Chronic Tears of the Achilles Tendon: A Long-Term Follow-up Study
- Free Gracilis Tendon Graft for Reconstruction of Chronic Tears of the Achilles Tendon