

- Discussion:
- coverts a complex link joint to a simple hinge by creating a radiocarpal articulation;
- motion between the radius and capitate is both translational and rotational, which has the effect of dissipating forces on the radius;
- expect 60-80% of contralateral motion (w/ about an 80% flexion-extension arc);
- expect preservation of about 70-100% of contra-lateral grip strength;
- patients w/ SLAC wrist or w/ scaphoid nonunion can expect significant pain relief (when capitolunate arthrosis is not present);
- even patients that perform heavy work can expect good results w/ this procedure;
- advantages of PCR are that it is technically easy, and often allows better preservation of strength and motion, as compared to
limited carpal arthrodesis;
- also, the great majority of patients can expect dramatic relief of pain (which by itself will often allow patients greater return of
function and strength;
- disadvantages: causes relative lengthening of extrinsic tendons and possibility of incongruity between the capitate and the lunate;
- outcome studies:
- in the report by Cohen and Kozin (2001) the authors compared proximal row carpectomy to 4 corner fusions;
- 2 cohort populations of 19 patients from separate institutions performing either a scaphoid excision and 4-corner arthrodesis;
- at the follow-up exam wrist motion revealed no significant differences in the flexion-extension arc, averaging 81° in PRC
patients and 80° following 4-corner arthrodesis, which was 62% and 58%, respectively, of the opposite wrist;
- 4-corner arthrodesis patients maintained greater radial deviation and total percent radial-ulnar deviation of the wrist;
- grip strength averaged 71% for the PRC group compared with 79% for the 4-corner arthrodesis patients;
- pain relief was similar using a variety of measures and patient satisfaction was equivalent.
- references:
- Degenerative arthritis of the wrist: proximal row carpectomy versus scaphoid excision and four-corner arthrodesis
- Proximal Row Carpectomy: Minimum 20-Year Follow-Up
- Indications:
- advanced scapholunate dissociation (see SLAC)
- dorsiflexion instability
- nonunion of scaphoid (w/ carpal instability)
- failed silicone lunate implant arthroplasty;
- Kienbock's disease;
- proximal row carpectomy may not be appropriate for Kienböck disease since lunate collapse damages the joint surfaces of the
capitate and radius;
- Technique:
- dorsal longitudinal approach thru the third compartment;
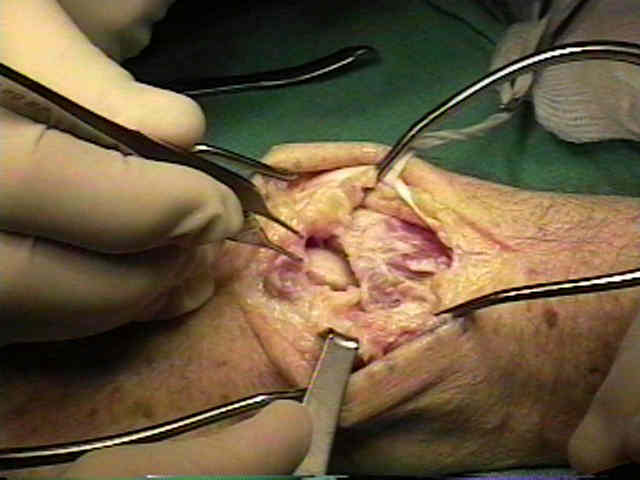
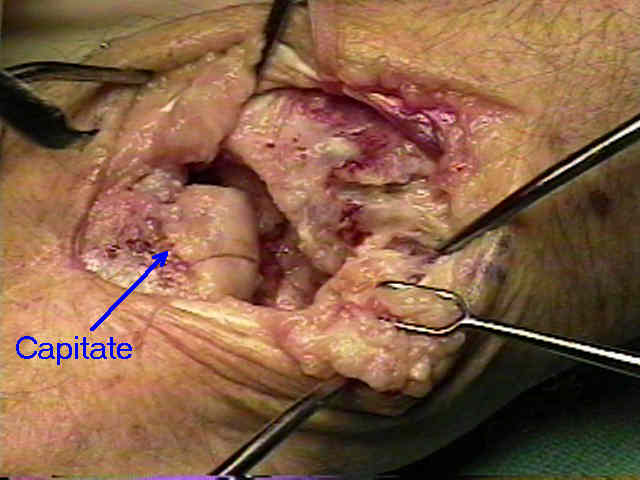
- lunate fossa and head of the capitate were inspected for degenerative changes.
- preserve the radioscaphocapitate ligament: (see wrist ligaments)
- prevents ulnar subluxation after proximal row carpectomy;
- having the surgical assistant apply traction on the index and long fingers will facilitate excision of the proximal carpal row;
- use small rongeurs to excise the middle of each bone, which allows the proximal and distal edges of the proximal carpal bones to
collapse together, making it easier to excise the remaining bone ends along their peripheral edges;
- during carpal excision, take care to avoid injury to palmar wrist ligaments, TFCC, capitate and pisiform;
- assess whether there is incongruity between the capitate and the lunate fossa of the distal radius;
- limitation of radial deviation may be a common postoperative finding;
- if impingement is observed at the time of surgery, then a radial styloidectomy should be considered;
- in most cases a radial styloidectomy will probably not be necessary;
- Post Op Care:
- classic teaching dictates three weeks of immobilization in a cast (need to avoid instability);
- if significant scarring is present from previous surgery, then consider shorter immobilization





 - Contraindications:
- Contraindications:
- if there is evidence of arthritic change in the lunate fossa and/or proximal involvement of the head of the capitate;
Proximal row carpectomy: a multicenter study.
Surgical Treatments for Scapholunate Advanced Collapse Wrist: Kinematics and Functional Performance
On resection of the proximal carpal row.
Proximal row carpectomy for posttraumatic disorders of the carpus.
Proximal-row carpectomy for diseases of the proximal row.
Proximal row carpectomy: Clincial evaluation.
Long-term results following proximal row carpectomy
Proximal-row carpectomy. An end-result study of twenty-two cases.
Proximal row carpectomy: A minimum 10-year follow-up study.
Proximal Row Carpectomy. Study with a Minimum of Ten Years of Follow-up.