

- See: Pediatric Elbow Injuries
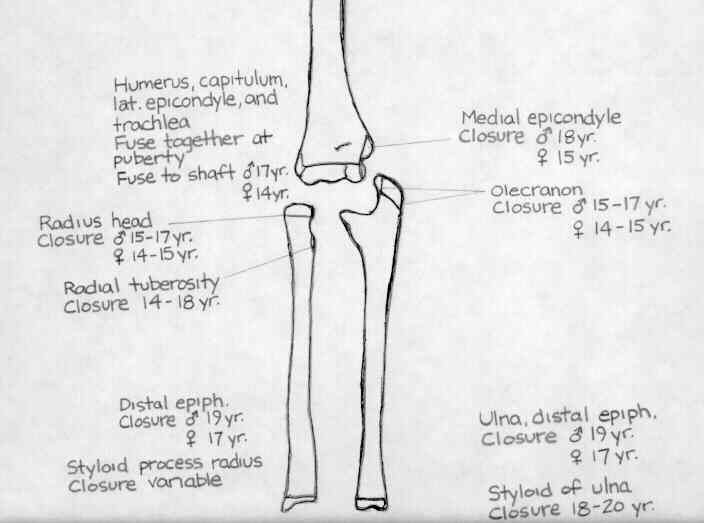
- Ossification Centers of the Elbow:
- C apetellum (appears age 1-2)
- R adial Head (appears age 2-4)
- I nteranal epicondyle (appears age 4-6)
- T rochlea (appears age 8-11)
- O lecranon (9-11 years)
- E xternal epicondyle (appears age 10-11)
- AP View:
- medial and lateral epicondyles and humeral-ulnar/radial articulation;
- carrying angle;
- if flexion contracture is present, 2 AP views should be taken, one perpendicular to the forearm and one perpendicular to humerus;
- technique: AP
- forearm is positioned supine (palm up) on the table;
- elbow joint is fully extended and the fingers slightly flexed;
- central beam is directed perpendicular to the elbow joint;
- AP views with the beam perpendicular to the proximal forearm and perpendicular to the distal humerus should be obtained;
- Lateral View:
- forearm flexed to 90;
- line from radial head to capitulum;
- film should demonstrate trochlea & capitellum overlapping w/ space between the humerus and the radial head;
- soft tissue structures:
- anterior fat pad:
- superficial part of anterior fat pad should be in front of coronoid fossa;
- in normal elbow the anterior fat pad should be barely visualized;
- look for small radiolucent area between bony rim & moderate opaque shadows of brachialis;
- w/ joint effusion (2nd to a minimally displaced radial head frx) there will be anterior & superior displacement of
anterior fat pad;
- posterior fat pad should not be seen at all;
- w/ a posterior fat pad sign and no obvious frx, obtain an oblique radiograph to help rule out supracondylar or lateral condyle frx;
- Skaggs DL and Mirzayan R (1999): prospectively examined a group of children with acute elbow trauma and a posterior
fat pad sign, but no evidence of radiographic fracture;
- at three weeks, new radiographs were taken and were evaluated for signs of fracture healing;
- they found that 34 out of 45 patients (76%) had evidence of a fracture.
- 53% of patients had supracondylar frx, 26% had a proximal ulnar frx, 12% had a frx of the lateral condyle, and 9%
had a frx of the radial neck;
- the authors conclude that children w/ a history of acute elbow trauma and a posterior fat pad sign, should be treated
as if they have a non displaced frx about the elbow;
- The Posterior Fat Pad Sign in Association with Occult Fracture of the Elbow in Children
- technique:
- forearm rests on its ulnar side on cassette w/ elbow flexed 90 deg;
- central beam is directed vertically toward the radial head;
- Internal oblique:
- trochlear notch of ulna and tip of olecranon process;
- shows medial epicondyle and coronoid process of ulna;
- External oblique:
- capitulum and head of radius; proximal radioulnar joint;
- Misc Features:
- radiocapitellar articulation: axis of radius should poiont toward center of capitellum on all views;
- when this relationship is disrupted consider:
-
- elbow dislocation;
- lateral condyle fracture;
- Monteggia Frx
The Posterior Fat Pad Sign in Association with Occult Fracture of the Elbow in Children
Radiology of postnatal skeletal development. VI. Elbow joint, proximal radius, and ulna.
Radiology of postnatal skeletal development. V. Distal humerus.
Limitations of the Radiocapitellar Line for Assessment of Pediatric Elbow Radiographs