

- Lateral Approach:
- incision is made directly lateral in thigh & thru midpoint of lateral condyle distally, staying anterior to proximal insertion of LCL;
- proximal exposure:
- incision is extended as necessary for diaphyseal involvement of the supracondylar frx;
- distal exposure:
- incision extends across the knee joint to a point distal and lateral to the tibial tubercle;
- thru the intermuscular septum;
- indentify superior lateral geniculate artery, which often requires ligation;
- incise thru the joint capsule but avoid damage to the lateral meniscus;
- avoid medial stripping and avoid posterior dissection (beware of posterior N/V bundle);
- extensile exposure:
- limited medial parapatellar arthrotomy:
- incision needs to be kept medial to avoid a narrow skin bridge and skin necrosis;
- patellar can be retracted laterally, giving excellent exposure of the femoral condyles;
- tibial tubercle osteotomy:
- if further exposure is needed, incision is extended distally to a point just lateral to the tibial tuberosity;
- before osteotomy, the tubercle is drilled and tapped;
- osteotomy of tuberosity may be performed and its attached patellar tendon and the entire quadriceps mechanism is refleced;
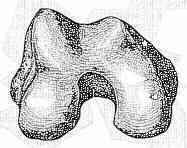
- place a blunt Hohmann retractor across the joint and over medial femoral condyle inorder to visualize articular surfaces of
medial and lateral femoral condyles;
- after fixation of frx, block of tuberosity is replaced in its bed and stabilized w/ 6.5 mm cancellous screw, which engages posterior cortex;
- Chapman Anterolateral Approach:
- longitudinal midline skin incision is made;
- interval between the rectus femoris and the vastus lateralis is identified proximal to the conjoined tendon of the rectus femoris and the vastus intermedius;
- sheath of the rectus femoris is then incised, and the muscle is isolated with blunt dissection from the underlying vastus intermedius distally as far as the conjoined tendon;
- tendon is incised along its lateral border into the suprapatellar pouch, with the dissection carried distally to the tibial tubercle in a lateral parapatellar fashion;
- if a posterior exposure of the lateral femoral condyle is needed, the incision is extended through the joint capsule parallel and just anterior to the muscle fibers of the vastus lateralis (rather
than parallel to the patellar ligament);
- rectus femoris is retracted medially;
- thinnest portion of the vastus intermedius is identified and is split longitudinally in line with the distal exposure as far proximally as needed to perform the procedure;
- although this technique gives better lateral exposure, it limits the ability to reflect the patella medially;
- femur is exposed through subperiosteal dissection on its lateral and anterior surfaces, but care is taken not to expose or strip the posterior or medial surfaces
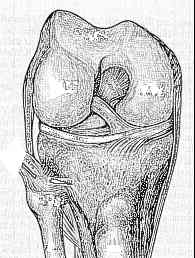
- Pertinent Anatomy for ORIF
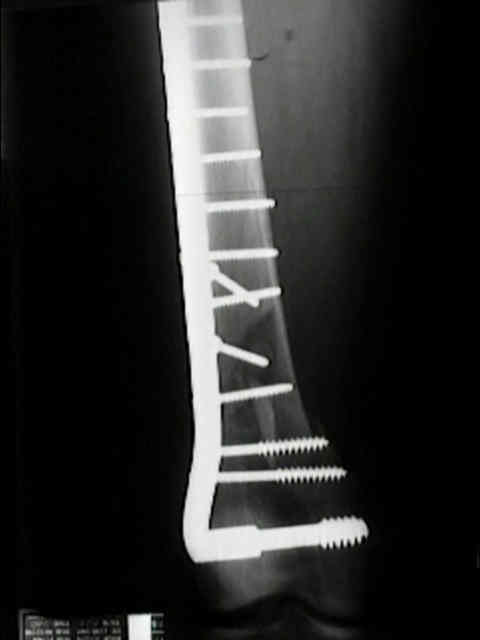
Treatment of Supracondylar Nonunions of the Femur with Plate Fixation and Bone Graft.