

- Discussion:
- most common error is non isometric anterior tunnel placement within intercondylar notch rather than at its normal posterior insertion; 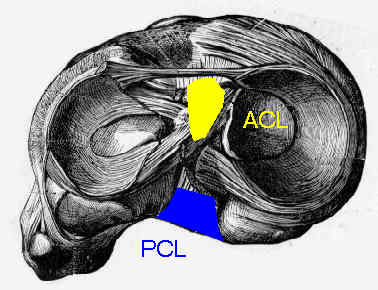
- ACL graft should pull up into tibial tunnel by about 2mm with extension when fixed on femoral side;
- this represents the closest reconstitution of the ACL's "physiometry"; (see: isometry);
- graft that tightens (pulls up into the tibial tunnel) with flexion will have a much higher likelyhood of failure and usually indicates a
femoral tunnel too far anterior in the notch;
- notchplasty
- Morphology of the Femoral Intercondylar Notch
- Editorial: The Lateral Intercondylar Ridge—A Key to Anatomic Anterior Cruciate Ligament Reconstruction
- Effects of notchplasty and femoral tunnel position on excursion patterns of an anterior cruciate ligament graft.
- tunnel positioning:
- anterior graft placement (relative to normal anatomical insertion of ACL) results in high strain on graft as knee is flexed;
- this restricts flexion of knee if graft remains intact, or it may elongate graft if the range of motion is restored;
- posterior placement or distal to normal site of attachment results in excessive tightening of the graft when knee is extended;
- consider whether there is an interplay between posterior graft placement and appropriate graft tension;
- with a posteriorly positioned femoral tunnel consider final tibial graft fixation in full extension rather than 30 deg flexion, since positioning
in 30 deg flexion at the time of final fixation may result in excessive graft tension when the knee is position in full extension;
- lateral tunnel placement:
- w/ a right knee, place the tunnel at about the 9:30 to 10 o’clock position;
- allows the femoral attachment point to overlap the anterolateral and posteromedial bundles insertion site
- in the report by Strobel MJ, et al., the authors report a case of a painful reflex extension loss due to femoral malplacement of an ACLgraft in a female high-level athlete;
- graft was placed on the femoral site in the high noon position combined with a slight medial tibial tunnel placement;
- resulting anterior-posterior cruciate ligament impingement near extension caused a persistent functional extension deficit of 20°;
- under anesthesia, the extension loss diminished, and thus it was hypothesized that the ACL-PCL impingement during extension activates a
proprioceptive reflex leading to a functional extension loss while the patient is awake.
- references:
- Reflex extension loss after anterior cruciate ligament reconstruction due to femoral "high noon" graft placement.
- Knee stability and graft function following anterior cruciate ligament reconstruction: Comparison between 11 o'clock and 10 o'clock femoral tunnel placement. 2002 Richard O'Connor Award paper.
- Knee stability and graft function after anterior cruciate ligament reconstruction: a comparison of a lateral and an anatomical femoral tunnel placement.
- Native Anterior Cruciate Ligament Obliquity Versus Anterior Cruciate Ligament Graft Obliquity. An Observational Study Using Navigated Measurements
- Femoral tunnel placement in single-bundle anterior cruciate ligament reconstruction: a cadaveric study relating transtibial lateralized femoral tunnel position to the anteromedial and posterolateral bundle femoral origins of the anterior cruciate ligament..
- Vertical femoral tunnel placement results in rotational knee laxity after anterior cruciate ligament reconstruction.
- Surgical Technique:
- one incision transtibial technique
- main criticism is that in some cases a transtibial tunnel will not allow for the exact desired tunnel placement (you get what you get)
- ref: Modified Transtibial Versus Anteromedial Portal Technique in Anatomic Single-Bundle Anterior Cruciate Ligament Reconstruction. Comparison of Femoral Tunnel Position and Clinical Results.
- two incision technique (outside in)
- open technique (which might be required with arthroscopy malfunction)
- anteromedial portal technique:
- this technique allows for a more anatomic and precise placement of the femoral tunnel (more reliable posterior placement);
- ACL position is lower and more horizontal than that achieved when performing the transtibial (TT) procedure.
- surgeon will also note more perpendicular drill angle to bone surface with AM vs TransTibial drilling;
- figure four flexed position assist with providing the best femoral target;
- increased risk of critically short tunnels (<25 mm) and posterior tunnel wall blowout when a conventional offset guide is used
- make sure that interference screws are less than 25 mm in length;
- ref: Correlation between femoral tunnel length and tunnel position in ACL reconstruction.
- references:
- Femoral Tunnel Drilling From the Anteromedial Portal Using the Figure-4 Position in ACL Reconstruction.
- A Comparison of 2 Drilling Techniques on the Femoral Tunnel for Anterior Cruciate Ligament Reconstruction
- Can anatomic femoral tunnel placement be achieved using a transtibial technique for hamstring anterior cruciate ligament reconstruction?
- Drilling the Femoral Tunnel During ACL Reconstruction: Transtibial Versus Anteromedial Portal Techniques.
- Femoral bone tunnel placement using the transtibial tunnel or the anteromedial portal in ACL reconstruction: a radiographic evaluation
- Transtibial versus anteromedial portal of the femoral tunnel in ACL reconstruction: a cadaveric study
- The relationship between femoral tunnels created by the transtibial, anteromedial portal, and outside-in techniques and the anterior cruciate ligament footprint
- Anatomic femoral tunnel drilling in anterior cruciate ligament reconstruction: use of an accessory medial portal versus traditional transtibial drilling
- Anteromedial Portal vs Transtibial Drilling Techniques in Anterior Cruciate Ligament Reconstruction: Any Clinical Relevance? A Retrospective Comparative Study
- Modified transtibial versus anteromedial portal technique in anatomic single-bundle anterior cruciate ligament reconstruction: comparison of femoral tunnel position and clinical results.


- Complications:
- 30-year-old male who presented for revision ACL reconstruction;
- (his medical history and operative note were not available for review);
- the obvious teaching points are that both the femoral and tibial tunnels were placed far to anterior;
- another example of how not to perform an ACL reconstruction:

- historic techniques:
- over the top position:
- over the top repair tensioned in extension will provide support in terminal extension but may slacken at greater flexion angles;
- grafts that pass thru femoral tunnels develop more internal pressure at femoral attachment site than those passed over top because of sharp edge of the tunnel;
- some create a trough in the femur to bring graft closer to anatomical position, or they fix graft in place w/ knee in full extension;
Anterior cruciate ligament reconstruction with patellar tendon: an ex vivo study of wear-related damage and failure at the femoral tunnel.
Anterior cruciate ligament replacements: a mechanical study of femoral attachment location, flexion angle at tensioning, and initial tension.
ACL graft can replicate the normal ligament's tension curve.