

- See: Pediatric Femoral Frx Menu
- Discussion:
- timing:
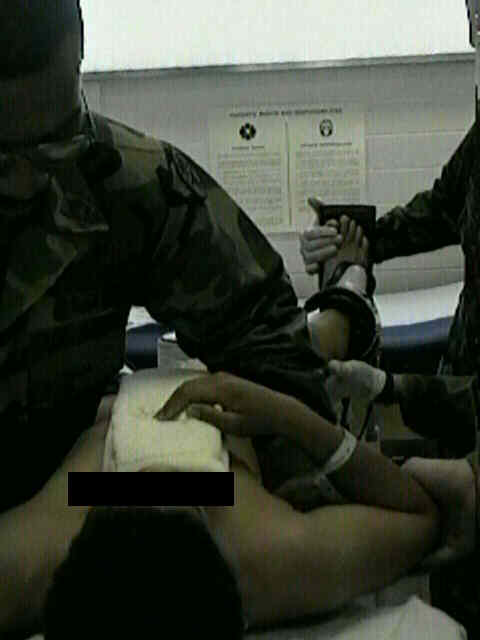
- Immediate single-leg spica cast for pediatric femoral diaphysis fractures.
- contraindications:
- unacceptable shortening or angulation;
- open fractures;
- thoracic or intra-abdominal trauma;
- large or obese children (inability for parents to care for child);
- position of spica:
- place affected thigh in 10 deg of abduction or in neutral position w/ opposite hip in moderate abduction to facilitate perineal hygiene;
- to decrease muscle forces & to minimize amount of shortening, place the lower extremity in the relaxed position;
- w/ hip flexion, abduction, external rotation & knee flexion;
- common mistake is to place the fractured thigh in marked abduction w/ resulting lateral bowing due to the pull of strong adductors;
- consider placing the limb in the correct position before application of spica;
- proximal 1/3 frx:
- hip flexion : 45 deg
- hip abduction: 30 deg
- ext rotation: 20 deg
- mid shaft fractures:
- hip flexion: 30 deg
- hip abduction: 20 deg
- ext rotation: 15 deg
- distal 1/3 frx:
- hip flexion: 20 deg
- hip abduction: 20 deg
- ext rotation: 15 deg
- Technique:
- technique pearls: padding:
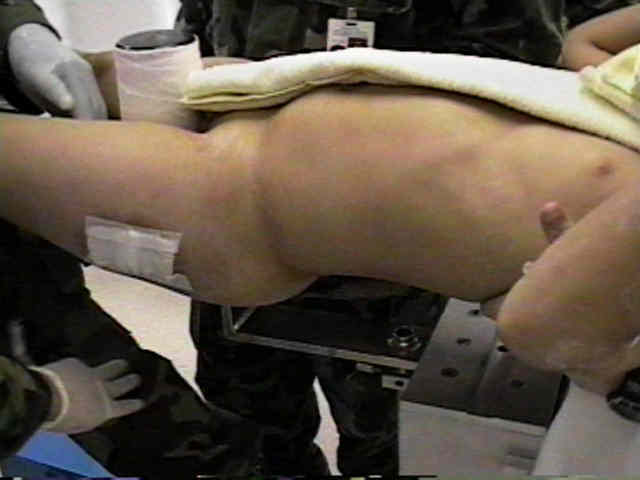
- place a folded towel on the anterior thorax and abdomen and apply all padding and casting material over this towel;
- following cast application the towel is removed;
- this will create space between the cast and the thorax/abdomen and will avoid cast tightness and difficult w/ breathing;
- using this technique, it is not necessary to window the abdomen of the cast;
- its useful to place 2 layers of body stockingette over the patient's torso to ensure that the cast padding can be pulled up over
the edges of the cast;
- gortex soft wrap is preferable to cotton wrap (gortex can be cleaned if it gets soiled);
- soft wrap (preferably Gortex) is placed, w/ care to evenly spread the cotton across the back and buttochs (including sacrum);
- a thick belt of felt is taped across the chest, just below the nipple line;
- a second felt belt is fashioned to cover the sacrum, PSIS, and ASIS;
- reduction:
- prior to cast application, use flouro to help determine the optimal position for reduction;
- distal femoral traction pin is inserted if fracture needs to be brought out to length;
- apply the cast, but apply minimal cast material around the injured thigh;
- once the cast is hard, bring in flouro and determine if the reduction is adequate;
- if the reduction is not adequate, then circumferentially cut the cast at the level of the frx;
- then re-reduce the fracture under flouroscopic control;
- once the reduction is adequate, have an assistant quickly apply more casting material while the thigh is held in the reduced position;
- cast re-enforcement:
- apply a "broom stick" between the thighs and apply cast material over this, inorder to strengthen the cast and prevent cast
breakdown at the hip joint;
- Cast Care:
- goretex liner allows the child and the cast to be washed;
- a panty shield napkin can be applied to the perineum to prevent soiling of the cast;
- child is seen every 2 weeks for evidence of skin break down







- references:
- Modified functional bracing in the ambulatory treatment of femoral shaft fractures in children.
- Functional fracture-bracing of long-bone fractures of the lower extremity in children.
- Long-term results in the treatment of femoral-shaft fractures in young children by immediate spica immobilization.
- Improved treatment of femoral shaft fractures in children. The "pontoon" 90-90 spica cast.
- Early spica cast management of femoral shaft fractures in young children. A technique utilizing bilateral fixed skin traction
- Immediate spica cast system for femoral shaft fractures in infants and children.
- Rotational deformity and remodeling after fracture of the femur in children.
- Incidence of skin complications and associated charges in children treated with hip spica casts for femur fractures.
- Comparison of titanium elastic nails with traction and a spica cast to treat femoral fractures in children.
- Single-Leg Spica Cast Application for Treatment of Pediatric Femoral Fracture
Improved treatment of femoral shaft fractures in children. The "pontoon" 90-90 spica cast.
Immediate spica cast system for femoral shaft fractures in infants and children.