

- See: Fracture Dislocation
- Discussion:
- isolated displaced greater tuberosity fractures are thought to occur in less than 2% of proximal humeral frx;
- greater tuberosity fragments w/ its attached rotator cuff will characteristically have a longitudinal tear in the cuff between the supraspinatus and subscapularis tendons;
- additionally, displaced fractures are associated w/ longitudinal rotator cuff tears;
- note that these fractures are often associated w/ anterior shoulder dislocation;
- in some cases, the magnitude of the fracture defect in the humeral head will be over-estimated due to the presence of an unrecognized Hill Sachs lesion;
- nerve injury:
- in the presentation by A. Garg et al (15 th OTA meeting), the authors noted 16 nerve injuries out of 50 patients w/ greater tuberosity frx;
- nerve injuries included: 10 axillary, 3 brachial plexus injuries, 1 median, and 1 ulnar nerve injury;
- Non Operative Treatment:
- greater tuberosity fractures are usually retracted posteriorly & superiorly, and closed reduction is difficult;
- this retraction may recur after reduction;
- if left in this position, impingment will develop against the acromion, limiting elevation and external rotation of the shoulder;
- if frx is assoc w/ anterior dislocation, closed reduction of glenohumeral dislocation may successfully reduce greater tuberosity fracture;
- once the tuberosity fragment has healed, recurrent anterior instability is unlikely;
- Indications for Surgery:
- presence of a mechanical block to reduction;
- post reduction displacement > 5 - 10 mm in any plane requires ORIF;
- axillary view usually shows the most significant displaced, but in some cases CT scan may be indicated to accurately determine amount of displacement;
- note that 5 mm of displacement might end up causing impingement in younger patients;
- Operative Treatment:
- anterior approach to the shoulder provides the best exposure;
- remember that the rotator cuff will cover the posterior and superior poritons of the greater tuberosity fragment, which therefore means that only the antero-inferior portion of the fragment is visible for reduction;
- this antero-inferior portion of the fragment may not be well visualized by deltoid splitting incisions (such as used in rotator cuff repairs);
- alternatively consider a "rotator cuff" type incision:
- 5 cm incision is made parallel to the skin creases over the anterosuperior protion of the shoulder;
- deltoid is split 4 cm along the anterosuperior raphe of the deltoid (further splitting may injure the axillary nerve);
- fixation:
- the tuberosity fragment is reduced and secured to its bed using heavy non absorbable sutures, either using a McGowen needle or through drill holes;
- occassionally, cancellous lag screws with washers may be used to achieve stable fixation;
- subsequently the longitudinal tear in the rotator cuff is repaired;
- this tear is characteristically located in the interval between the supraspinatus and the subscapularis muscles;
- Case Example of Frx Dislocation:


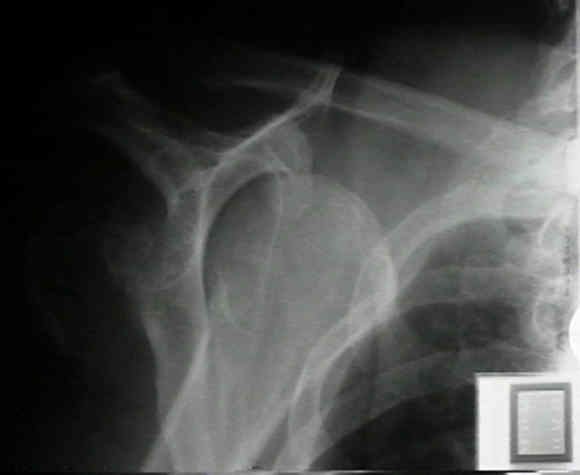



- 27 year old female who sustained a greater tuberosity frx - anterior dislocation during a seizure;
- she underwent ORIF of the fragment using No 5 Ethibond sutures and two screws;
- note the large Hill Sachs fragment;



Year Book: Open Reduction and Internal Fixation of Two-Part Displaced Fractures of the Greater Tuberosity of the Proximal Part of the Humerus.